Hospice Billing Manual
- Hospice Care
- Billing Information
- Hospice Benefits
- Revenue Coding
- Post Eligibility Treatment of Income (PETI) Nursing Facility Supplemental Benefits
- Date of Death or Date of Discharge (DOD)
- UB-04 Paper Claim Reference Table
- Timely Filing
- Institutional Provider Certification
- Early and Periodic Screening, Diagnosis and Treatment
- Removal of Electronic Visit Verification from Hospice
- Hospice Revisions Log
Return to Billing Manuals Web Page
Hospice Care
Providers must be enrolled as a Health First Colorado (Colorado's Medicaid program) provider in order to:
- Treat a Health First Colorado member
- Submit claims for payment to Health First Colorado
Hospice services are available to Health First Colorado members with a terminal illness (life expectancy of nine [9] months or less). Palliative treatment includes services and interventions that are not curative but provide the greatest degree of relief and comfort for the symptoms of the terminal illness.
Providers should refer to the Code of Colorado Regulations, Program Rules (10 C.C.R. 2505-10), for specific information when providing hospice care.
Billing Information
Refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down for general billing information.
Hospice Benefits
The member may receive Health First Colorado Hospice Benefit (MHB) services in a:
- Private residence
- Residential care facility (Alternative Care)
- Licensed hospice facility
- Intermediate Care Facility for Individuals with Intellectual Disability (ICF-IDD)
- Skilled Nursing Facility (SNF)
- Nursing Facility (NF)
- Effective May 3, 2024, place of service 03 is an allowed place of service for all fee-for-service benefits. In order for community providers to bill fee-for-service to children in a school setting, the provider must follow school district policy. Please reference the Community Providers in a School Setting Policy memo.
Health First Colorado Hospice Benefit members residing in a nursing facility must meet hospice level of care and financial Health First Colorado eligibility criteria.
Hospice SNF/NF room and board reimbursement is made to the hospice provider for each home care level day (routine or continuous care).
- The member must choose MHB services.
- The member's attending physician must certify that the member is terminal.
- Both the member and the attending physician must agree to the plan of care developed by the hospice provider.
- A participating MHB provider must provide all MHB services.
- Hospice services are co-payment exempt.
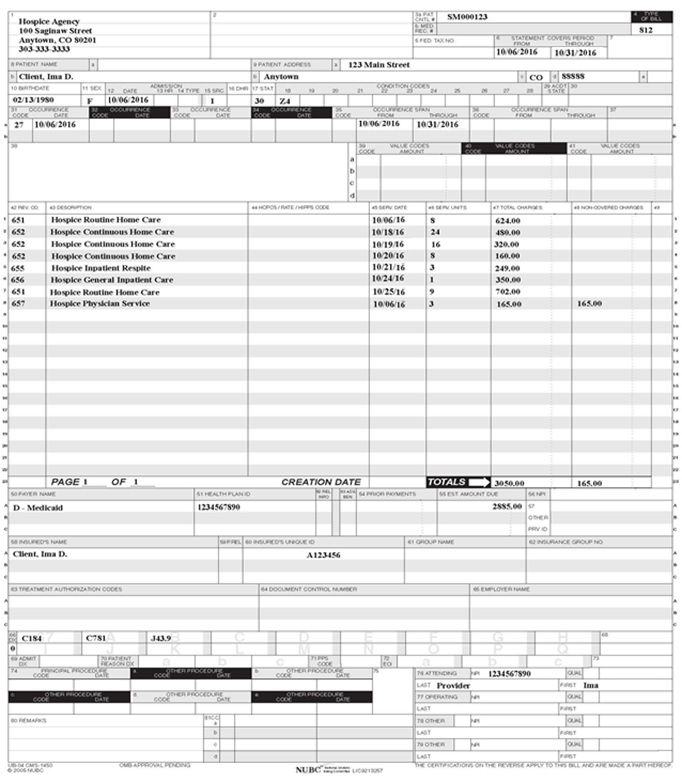
- Physician services are not a covered MHB, they are billed by the physician as a regular physician service.
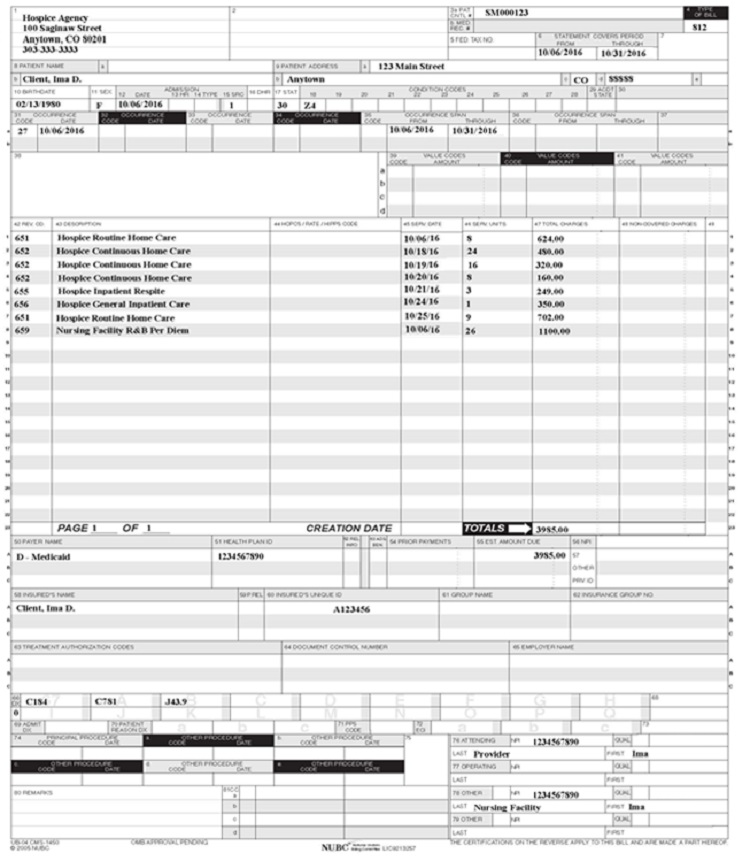
- The SNF/NF provides the hospice with the room and board per diem amount for hospice members residing in an SNF/NF. The hospice bills room and board on behalf of the member to Health First Colorado which reimburses 95% of the per diem amount, and the hospice passes the room and board payment through to the SNF/NF.
The patient liability amount may apply when a hospice member resides in an NF. This is payment made by the member for NF care, after the personal needs allowance and other approved expenses are deducted from member income. The personal needs allowance and other approved deductions are determined by County Income Maintenance Technicians. The patient liability amount must be applied to the member's care.
When reporting the patient liability amount for the entire month, regardless of the number of days in that month, apply the total patient liability.
Example:
Bill the full $100.00 (Per Diem Rate) amount
The processing system automatically deducts 5% - $100 X .95= $95.00
$95.00 X 31 = $2,945.00
$2,945.00 - $500.00 = $2,445.00 (NF R and B)
$2,445.00 + $3,500.00 (routine home care amount) = $5,945.00 Total Reimbursement.
Use the per diem calculation to calculate the correct amount when reporting the patient liability amounts for less than one full month of NF care. The per diem calculation is the number of days in the facility, excluding the date of discharge, times the facility per diem rate.
To Calculate NF Partial Patient Liability:
- Calculate the Health First Colorado amount by multiplying the number of days for payment times the per diem amount.
- If the Health First Colorado amount exceeds the patient liability amount, the partial month's patient liability amount remains the same as the regular patient liability amount.
- If the patient liability is more than the Health First Colorado amount, the partial month's patient liability is the same as the Health First Colorado amount. The excess of the patient liability over the partial month's patient liability belongs to the resident and, if it has already been paid to the facility, shall be refunded to the resident. It is the SNF's/NF's responsibility to collect patient liability. The hospice does not have to collect patient liability. The hospice may choose to collect this amount and pay the SNF/NF.
Revenue Coding
Bill Hospice services with the following revenue codes:
| Service | Revenue Code | Description |
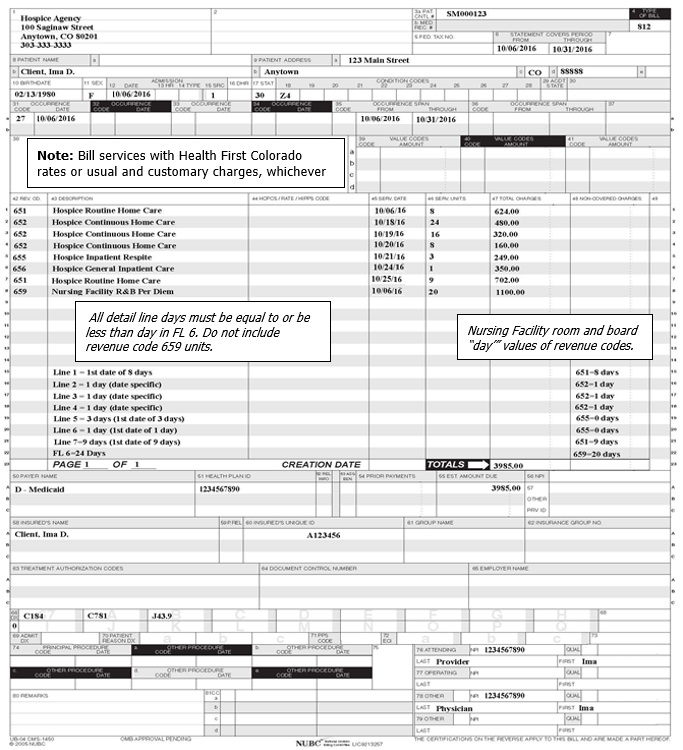
| Hospice Routine Home Care | 650 651 | Care Days 1-60 One Unit = 1 day Care Days 61+ One Unit = 1 day |
| Continuous Home Care | 652 | One Unit=1 hour (must be at least 8 hours in a 24-hour period with more than half provided by a nurse) |
| Service Intensity Add-on Hospice Inpatient Respite | 652 655 | One Unit=1 hour (up to 4 hours and member must be seen by a nurse or social worker within the last 7 days of life) One Unit = 1 day |
| Hospice General Inpatient Care | 656 | One Unit = 1 day |
| Hospice Physician Service (Visit) | 657 | One Unit = 1 visit Non-covered MHB service (Non-covered charges must be shown in both FL 53 and 54.) |
| Hospice NF Room and Board Per/Diem | 659 | One unit = 1 day |
Post Eligibility Treatment of Income (PETI) Nursing Facility Supplemental Benefits
Post Eligibility Treatment of Income (PETI) is defined as the reduction of resident payment to a nursing facility for costs of care provided to an individual for services not covered by the Medical Assistance Program, by the amount that remains after certain approved deductions are applied and paid to the providers to reduce the individual's total payment.
- The individual is liable to pay the remaining amount to the institution.
- Members who reside in a nursing facility, are receiving hospice services and who are making a patient liability payment must have a letter from their primary care physician stating why these additional services are medically necessary and requested by the resident.
- These requests will be considered individually, and the Department of Health Care Policy & Financing (the Department) will determine whether or not to approve the request.
- The Long-Term Care (LTC) facility or the family determines the need for Non-Medical Assistance Program covered services.
- The facility or family arranges for the member to see the provider.
All PETI expenses must be prior authorized by the Department. Prior Authorization Requests (PARs) should be sent to:
PETI Program
Department of Health Care Policy & Financing
303 E. 17th Avenue
Suite 1100
Denver, CO 80203
| PETI Revenue Codes | |||
| 479 | Hearing | 969 | Dental |
| 962 | Vision | 999 | Health Insurance/Other |
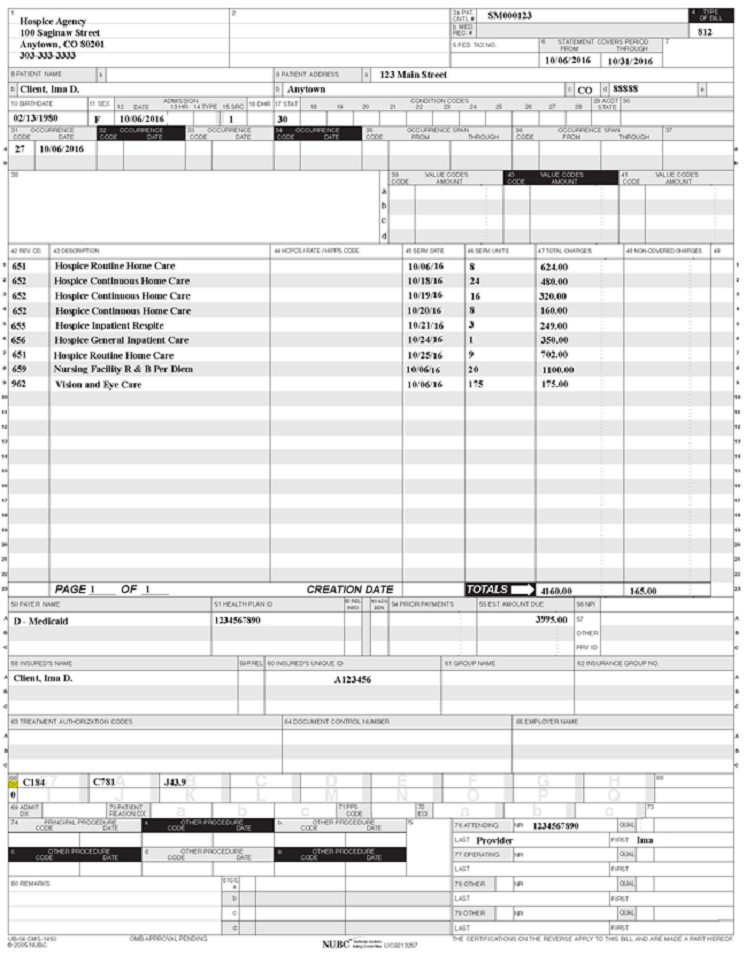
Hospice agencies are responsible for adding PETI codes to their claims for Medical Assistance Program members living in nursing facilities and who also make a patient liability payment. Once the charges are approved, the hospice agency may submit claims for the PETI payment on the claim with the member's room and board minus patient liability amount. The claims processing system will automatically complete the calculations.
Bill PETI charges in units. One unit equals one dollar.
Example with Claim: If a member has been approved for the purchase of eyeglasses at a cost of $175, the PETI amount equals 175 units at $1.00 each. Do not bill partial units or cents.
Date of Death and Date of Discharge (DOD)
Payment is made for the date of death and day of discharge (DOD). Home care rate applies if discharge is from general or respite inpatient care unless the member dies at an inpatient level of care. Inpatient level of care is paid at the applicable general or respite rate for the discharge date.
Payment for NF residents is made for services delivered up to the date of discharged (alive or deceased) and includes the applicable per diem payment for DOD. For the month of the member’s death, the following are allowed: Durable Medical Rental Equipment and oxygen.
UB-04 Paper Claim Reference Table
The information in the following table provides instructions for completing form locators (FL) as they appear on the paper UB-04 claim form. Instructions for completing the UB-04 claim form are based on the current National Uniform Billing Committee (NUBC) UB-04 Reference Manual. Unless otherwise noted, all data form locators on the UB-04 have the same attributes (specifications) for Health First Colorado as those indicated in the NUBC UB-04 Reference Manual.
All code values listed in the NUBC UB-04 Reference Manual for each form locator may not be used for submitting paper claims to Health First Colorado. The appropriate code values listed in this manual must be used when billing Health First Colorado.
The UB-04 Certification document must be completed and attached to all claims submitted on the paper UB-04. Completed UB-04 paper Health First Colorado claims, including hardcopy Medicare claims, should be mailed to the correct fiscal agent address listed in Appendix A located on the Billing Manuals web page under the Appendices drop-down.
Do not submit "continuation" claims. Each claim form has a set number of billing lines available for completion. Do not crowd more lines on the form.
Billing lines in excess of the designated number are not processed or acknowledged. Claims with more than one (1) page may be submitted through the Provider Web Portal.
Bill with a date span (From and To dates of service) only if the service was provided every consecutive day within the span. The From and To dates must be in the same month.
The Paper Claim Reference Table below lists the required, optional and/or conditional form locators for submitting the paper UB-04 claim form to Health First Colorado for nursing facility services.
| Form Locator and Labels | Completion Format | Instructions | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Billing Provider Name, Address, Telephone Number | Text | Required
Abbreviate the state using standard post office abbreviations. Enter the telephone number. | ||||||||||||||||||||||||||||||||||||||
| 2. Pay-to Name, Address, City, State | Text | Required only if different from FL 1.
| ||||||||||||||||||||||||||||||||||||||
| 3a. Patient Control Number | Up to 20 characters: Letters, numbers or hyphens | Optional Enter information that identifies the member or claim in the provider's billing system. Submitted information appears on the Remittance Advice (RA). | ||||||||||||||||||||||||||||||||||||||
| 3b. Medical Record Number | 17 digits | Optional Enter the number assigned to the member to assist in retrieval of medical records. | ||||||||||||||||||||||||||||||||||||||
| 4. Type of Bill | 3 digits | Required Use the following code range for Hospice: 811-815 for non-hospital-based Hospice services 821-825 for hospital-based Hospice services The three (3)-digit code requires one (1) digit from each of the sequences (Type of facility, Bill classification, and Frequency). Enter the three (3)-digit number indicating the specific type of bill. The three (3)-digit code requires one (1) digit each in the following sequences: Digit 1 Type of Facility: 8 - Special Facility (Hospice) Digit 2 Bill Classification (Special facilities Only): 1 - Hospice (Non-Hospital Based) 2 - Hospice (Hospital Based) Digit 3 Frequency: 0 - Non-Payment/Zero Claim 1 - Admit Through Discharge Claim 2 - Interim - First Claim 3 - Interim - Continuous Claim 4 - Interim - Last Claim 5 - Late Charge(s) Only Claim | ||||||||||||||||||||||||||||||||||||||
| 5. Federal Tax Number | None | Submitted information is not entered into the claim processing system. | ||||||||||||||||||||||||||||||||||||||
| 6. Statement covers period From/Through | From: 6 digits MMDDYY Through: 6 digits MMDDYY | Required "From" date is the actual start date of services. "From" date cannot be prior to the start date reported on the initial prior authorization, if applicable, or is the first date of an interim bill. "Through" date is the actual discharge date, or final date of an interim bill. "From" and "Through" dates cannot exceed a calendar month (e.g., bill 01/15/18 thru 01/31/18 and 02/01/18 thru 02/15/18, not 01/15/18 thru 02/15/18). Match dates to the prior authorization if applicable. If the member is admitted and discharged on the same date, that date appears in both form locators. Detail dates of service must be within the "Statement Covers Period" dates. | ||||||||||||||||||||||||||||||||||||||
| 8a. Patient Identifier | Text | Required Enter the Health First Colorado ID number for the member. | ||||||||||||||||||||||||||||||||||||||
| 8b. Patient Name | Up to 25 characters, letters and spaces | Required Enter the member's last name, first name and middle initial. | ||||||||||||||||||||||||||||||||||||||
| 9a. Patient Address - Street | Characters Letters and numbers | Required Enter the member's street/post office box as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||
| 9b. Patient Address - City | Text | Required Enter the member's city as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||
| 9c. Patient Address - State | Text | Required Enter the member's state as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||
| 9d. Patient Address - ZIP | Digits | Required Enter the member's zip code as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||
| 9e. Patient Address - Country Code | Digits | Optional | ||||||||||||||||||||||||||||||||||||||
| 10. Birthdate | 8 digits (MMDDCCYY) | Required Enter the member's birthdate using two (2) digits for the month, two (2) digits for the date, and four (4) digits for the year (MMDDCCYY format). Example: 01012010 for January 1, 2010. | ||||||||||||||||||||||||||||||||||||||
| 11. Patient Sex | 1 letter | Required Enter an M (male) or F (female) to indicate the member's sex. | ||||||||||||||||||||||||||||||||||||||
| 12. Admission Date | 6 digits | Required Enter the date care originally started from any funding source (e.g., Medicare, Health First Colorado, Third Party Resource, etc.). | ||||||||||||||||||||||||||||||||||||||
| 13. Admission Hour | 6 digits | Not Required | ||||||||||||||||||||||||||||||||||||||
| 14. Admission Type | 1 digit | Not Required | ||||||||||||||||||||||||||||||||||||||
| 15. Source of Admission | 1 digit | Required | ||||||||||||||||||||||||||||||||||||||
| 16. Discharge Hour | 2 digits | Not Required | ||||||||||||||||||||||||||||||||||||||
| 17. Patient Discharge Status | 2 digits | Required
*Hospice use only | ||||||||||||||||||||||||||||||||||||||
| 18-28. Conditions Codes | 2 digits | Required
| ||||||||||||||||||||||||||||||||||||||
| 29. Accident State | 2 digits | Not Required | ||||||||||||||||||||||||||||||||||||||
| 31 - 34. Occurrence Code/Date | 2 digits and 6 digits | Required
| ||||||||||||||||||||||||||||||||||||||
| 35-36. Occurrence Span Code From/ Through | Digits | Not Required | ||||||||||||||||||||||||||||||||||||||
| 38. Responsible Party Name/Address | None | Leave blank | ||||||||||||||||||||||||||||||||||||||
| 39 - 41. Value Codes and Amounts | 2 characters and up to 9 digits | Conditional
When member has Medicare "Part B only" coverage, and the provider is billing for the Health First Colorado Accommodation Per Diem and the payer source code is H, enter the "Part B only" ancillary services payment in this form locator on the Medicare line. | ||||||||||||||||||||||||||||||||||||||
| 42. Revenue Code | 4 digits | Required If billing for nursing facility per diem charges (Revenue Code 0659 or 0651), the nursing facility provider number must be entered in FL 78 (Other Phys. ID) Refer to the Revenue Coding table. | ||||||||||||||||||||||||||||||||||||||
| 43. Revenue code Description | Text | Required Enter the revenue code description or abbreviated description. | ||||||||||||||||||||||||||||||||||||||
| 44. HCPCS/Rates/ HIPPS Rate Codes | 5 digits | Not Required | ||||||||||||||||||||||||||||||||||||||
| 45. Service Date | 6 digits | Required For span bills only. Enter the date of service using MMDDYY format for each detail line completed. Each date of service must fall within the date span entered in FL 6 (Statement Covers Period). | ||||||||||||||||||||||||||||||||||||||
| 46. Service Units | 3 digits | Required Enter a unit value on each line completed. Use whole numbers only. Do not enter fractions or decimals and do not show a decimal point followed by a 0 to designate whole numbers. Example: Do not enter 1.0 to signify one (1) unit. For span bills, the units of service reflect only those visits, miles or treatments provided on dates of service in FL 45. | ||||||||||||||||||||||||||||||||||||||
| 47. Total Charges | 9 digits | Required Enter the total charge for each revenue code. For Medicare Part B claims, enter the total ancillary charges billed to Medicare. A grand total on line 23 is required for all charges. | ||||||||||||||||||||||||||||||||||||||
| 48. Non-covered Charges | Up to 9 digits | conditional Enter incurred charges that are not payable by Health First Colorado. Non-covered charges must be entered in both FL 47 (Total Charges) and FL 48 (Non-Covered Charges.) Each column requires a grand total. | ||||||||||||||||||||||||||||||||||||||
| 50. Payer Name | 1 letter and text | Enter the payment source code followed by name of each payer organization from which the provider might expect payment.
| ||||||||||||||||||||||||||||||||||||||
| 51. Health Plan ID | 10 digits | Required Enter the provider's Health Plan ID for each payer name. Enter the Health First Colorado number assigned to the billing provider. Payment is made to the enrolled provider or agency that is assigned this number. | ||||||||||||||||||||||||||||||||||||||
| 52. Release of Information | N/A | Submitted information is not entered into the claim processing system. | ||||||||||||||||||||||||||||||||||||||
| 53. Assignment of Benefits | N/A | Submitted information is not entered into the claim processing system. | ||||||||||||||||||||||||||||||||||||||
| 54. Prior Payments | Up to 9 digits | Conditional Complete when there are Medicare or third-party payments. Enter third party and/or Medicare payments. | ||||||||||||||||||||||||||||||||||||||
| 55. Estimated Amount Due | Up to 9 digits | Conditional Complete when there are Medicare or third-party payments. Enter the net amount due from Health First Colorado after provider has received other third party, Medicare or member liability amount. Medicare Crossovers Enter the sum of the Medicare coinsurance plus Medicare deductible less third-party payments and member payments. | ||||||||||||||||||||||||||||||||||||||
| 56. National Provider Identifier (NPI) | 10 digits | Required Enter the billing provider's 10-digit National Provider Identifier (NPI). | ||||||||||||||||||||||||||||||||||||||
| 57. Other Provider ID | Not Required | |||||||||||||||||||||||||||||||||||||||
| 58. Insured's Name | Up to 30 characters | Required Enter the member's name on the Health First Colorado line. Other Insurance/Medicare Complete additional lines when there is third party coverage. Enter the policyholder's last name, first name, and middle initial. | ||||||||||||||||||||||||||||||||||||||
| 60. Insured's Unique ID | Up to 20 characters | Required Enter the insured's unique identification number assigned by the payer organization exactly as it appears on the health insurance card. Include letter prefixes or suffixes shown on the card. | ||||||||||||||||||||||||||||||||||||||
| 61. Insurance Group Name | 14 letters | Conditional Complete when there is third party coverage. Enter the name of the group or plan providing the insurance to the insured exactly as it appears on the health insurance card. | ||||||||||||||||||||||||||||||||||||||
| 62. Insurance Group Number | 17 digits | Conditional Complete when there is third party coverage. Enter the identification number, control number, or code assigned by the carrier or fund administrator identifying the group under which the individual is carried. | ||||||||||||||||||||||||||||||||||||||
| 63. Treatment Authorization Code | Up to 18 characters | Conditional Complete when the service requires a PAR. Enter the authorization number in this FL if a PAR is required and has been approved for services. ASs of March 1, 2017, PETI/IMEs require a PAR. | ||||||||||||||||||||||||||||||||||||||
| 64. Document Control Number | None | Conditional | ||||||||||||||||||||||||||||||||||||||
| 65. Employer Name | Text | Conditional Complete when there is third party coverage. Enter the name of the employer that provides health care coverage for the individual identified in FL 58 (Insured Name). | ||||||||||||||||||||||||||||||||||||||
| 66. Diagnosis Version Qualifier | Submitted information is not entered into the claim processing system. Enter applicable ICD indicator to identify which version of ICD codes is being reported. 0ICD-10-CM (DOS 10/1/15 and after) | |||||||||||||||||||||||||||||||||||||||
| 67. Principal Diagnosis Code | Up to 6 digits | Required Enter the exact ICD-10-CM diagnosis code describing the principal diagnosis that exists at the time of admission or develops subsequently and affects the length of stay. Do not add extra zeros to the diagnosis code. | ||||||||||||||||||||||||||||||||||||||
| 67A. - 67Q. - Other Diagnosis | 6 digits | Optional Complete when there are additional conditions that affect treatment. | ||||||||||||||||||||||||||||||||||||||
| 69. Admitting Diagnosis Code | 6 digits | Required Enter the ICD-10-CM diagnosis code as stated by the physician at the time of admission. | ||||||||||||||||||||||||||||||||||||||
| 70. Patient Reason Diagnosis | Not Required | |||||||||||||||||||||||||||||||||||||||
| 71. PPS Code | Not Required | |||||||||||||||||||||||||||||||||||||||
| 72. External Cause of Injury code (E-Code) | 6 digits | Optional Enter the ICD-10-CM diagnosis code for the external cause of an injury, poisoning, or adverse effect. This code must begin with an "E". | ||||||||||||||||||||||||||||||||||||||
| 74. Principal Procedure Code/Date | 7 characters and 6 digits | Conditional Complete when there are additional significant procedure codes. Enter the ICD 10 CM procedure codes identifying all significant procedures other than the principal procedure and the dates on which the procedures were performed. Report those that are most important for the episode of care and specifically any therapeutic procedures closely related to the principal diagnosis. Enter the date using MMDDYY format. | ||||||||||||||||||||||||||||||||||||||
| 74A. Other Procedure Code/Date | 7 characters and 6 digits | Not Required | ||||||||||||||||||||||||||||||||||||||
| 76. Attending NPI - Required Attending Last/First Name | NPI - 10 digits Text | Health First Colorado ID Required NPI - Enter the 10-digit NPI number assigned to the physician having primary responsibility for the member's medical care and treatment. This number is obtained from the physician and cannot be a clinic or group number. (If the attending physician is not enrolled in Health First Colorado or if the member leaves the ER before being seen by a physician, the hospital may enter their individual numbers.) Hospitals and FQHCs may enter the member's regular physician's 10- digit NPI in the Attending Physician ID form locator if the locum tenens physician is not enrolled in Health First Colorado. QUAL - Enter "1D" for Health First Colorado Enter the attending physician's last and first name. This form locator must be completed for all services. | ||||||||||||||||||||||||||||||||||||||
| 77. Operating NPI | Optional Submitted information is not entered into the claim processing system. | |||||||||||||||||||||||||||||||||||||||
| 78 - 79. Other ID NPI - Conditional | NPI - 10 digits | Conditional Complete when attending physician is not the PCP or to identify additional physicians. Ordering, Prescribing, or Referring NPI - when applicable NPI - Enter up to two (2) 10-digit NPI numbers, when applicable. This form locator identifies physicians other than the attending physician. If the attending physician is not the PCP or if a clinic is a PCP agent, enter the PCP NPI number as the referring physician. The name of the Health First Colorado member's PCP appears on the eligibility verification. Review either for eligibility or PCP. Health First Colorado does not require that the PCP number appear more than once on each claim submitted. The attending physician's last and first name are optional. | ||||||||||||||||||||||||||||||||||||||
| 80. Remarks | Text | Enter specific additional information necessary to process the claim or fulfill reporting requirements. | ||||||||||||||||||||||||||||||||||||||
| 81. Code - QUAL/CODE/VALUE (a-d) | Qualifier: 2 digits Taxonomy Code: 10 digits | Optional Complete both the qualifier and the taxonomy code for the billing provider in field 81CC-a. Field 81CC-a must be billed with qualifier B3 for the taxonomy code to be captured in the claims processing system. If B3 is missing, no taxonomy code will be captured in the claims processing system. Only one (1) taxonomy code can be captured from field 81CC. If more than one (1) taxonomy code is provided, only the first instance of B3 and taxonomy code will be captured in the claims processing system. | ||||||||||||||||||||||||||||||||||||||
PETI Claim Example
Hospice Claim without Nursing Facility Room and Board with Physician Charges Example
Hospice Claim with Nursing Facility Room and Board Example
Hospice Claim with Patient Pay Example
Timely Filing
Refer to the General Provider Information Manual available on the Billing Manuals web page under the General Provider Information drop-down for more information on timely filing policy, including the resubmission rules for denied claims.
Institutional Provider Certification
The Institutional Certification form is available on the Provider Forms web page under the Claim Forms and Attachments drop-down menu.
Early and Periodic Screening, Diagnostic and Treatment
Hospice benefits are provided in accordance with Early and Periodic Screening, Diagnostic and Treatment (EPSDT) requirements as listed in 8.280.4.E: "Other EPSDT Benefits" 8.280.4.E reads as follows:
Other healthcare services may include other EPSDT benefits if the need for such services is identified. The services are a benefit when they meet the following requirements:
Providers can ask for these additional services by following the PAR process as outlined for this benefit.
- All goods and services described in Section 1905(a) of the Social Security Act are a covered benefit under EPSDT when medically necessary as defined at 10 C.C.R. 2505-10, Section 8.076.1.8, regardless of whether such goods and services are covered under the Colorado Medicaid State Plan.
- For the purposes of EPSDT, medical necessity includes a good or service that will, or is reasonably expected to, assist the client to achieve or maintain maximum functional capacity in performing one (1) or more Activities of Daily Living; and meets the criteria set forth at Section 8.076.1.8.b - g.
- The service provides a safe environment or situation for the child.
- The service is not for the convenience of the caregiver.
- The service is medically necessary.
- The service is not experimental or investigational and is generally accepted by the medical community for the purpose stated.
- The service is the least costly.
Visit the EPSDT web page for more information regarding EPSDT.
Contact Gina Robinson at Gina.Robinson@state.co.us with questions about EPSDT.
Removal of Electronic Visit Verification Requirement from Hospice
Effective July 1, 2024, the collection of EVV data will no longer be required for Hospice services.
Visit the EVV web page or refer to the EVV Program Manual for further information regarding the EVV program.
Contact EVV@state.co.us with any EVV questions.
Hospice Revision Log
| Revision Date | Section/Action | Made by |
|---|---|---|
| 12/1/2016 | Manual revised for interChange implementation. For manual revisions prior to 12/01/2016 Please refer to Archive. | HPE (now DXC) |
| 12/27/2016 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_2.xlsx. | HPE (now DXC) |
| 1/10/2017 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_3.xlsx. | HPE (now DXC) |
| 1/19/2017 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_4.xlsx. | HPE (now DXC) |
| 1/26/2017 | Updates based on Department 1/20/2017 approval email HPE (now DXC) | |
| 5/26/2017 | Updates based on Fiscal Agent name change from HPE to DXC | DXC |
| 6/15/2018 | Updated timely filing information and removed references to LBOD, removed general billing information already available in the General Provider Information manual | DXC |
| 6/27/2018 | Revision to timely filing | HCPF |
| 6/13/2019 | Updated Appendices' links and verbiage | DXC |
| 12/12/2019 | converted to web page | HCPF |
| 8/7/2020 | Updated item 81 of the Paper Claim Reference Table for taxonomy code billing | DXC |
| 9/13/2021 | Added sections for Payments to Licensed Hospice Facilities for Residential Care, Early and Periodic Screening, Diagnostic and Treatment (EPSDT), and Electronic Visit Verification | HCPF |
| 9/7/2022 | Removed "to the Health First Colorado for clarification purposes | HCPF |
| 2/14/2023 | Removal of out-of-date Payments to Licensed Hospice Facilities for Residential Care portion | HCPF |
| 8/16/2023 | Updated Department address | HCPF |
| 9/5/2023 | Removing SB 21-214 information | HCPF |
| 12/05/2023 | Changed ICF-MR to ICF-IID | HCPF |
| 4/23/2024 | Updated language concerning EVV | HCPF |
| 7/24/2024 | Add place of service 03 information | HCPF |
| 10/3/2024 | Addition of Date of Death or Date of Discharge (DOD) guidance | HCPF |