Emergency Medical Transportation Billing Manual
- Benefit Overview
- General Billing Information
- Eligible Providers
- Payment for Covered Services
- Member Eligibility
- Prior Authorization
- Covered Benefits and Limitations
- Procedure Coding
- EMT Billing Information
- CMS Paper Claim Reference Table
- Timely Filing
- EMT Billing Manual Revisions Log
Return to Billing Manuals Web Page
Benefit Overview
Emergency Medical Transportation (EMT) is a benefit for all Health First Colorado (Colorado's Medicaid program) members who have a critical or unknown illness or injury that demands immediate medical attention to prevent permanent injury or loss of life.
Providers must be enrolled as a Health First Colorado provider in order to:
- Provide EMT services to a Health First Colorado member
- Submit claims for payment to Health First Colorado
Providers should refer to the Code of Colorado Regulations (CCR), Program Rules (10 CCR 2505-10), for specific information when providing EMT services.
EMT Regulations can be found in 10 CCR 2505-10 8.018. These regulations allow inter-facility transfers between hospitals to be billed as EMT services. These transfers can include transportation of people who are experiencing a mental health or substance use disorder crisis.
General Billing Information
Refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down menu for general billing information.
Eligible Providers
To provide EMT services to Health First Colorado members and receive reimbursement, a provider must:
- Obtain the appropriate license, accreditation or recognition:
- Ground ambulances - Licensing of ground ambulance services in Colorado is conducted by county governments. Contact the county commissioner's office for specific county ambulance licensing requirements and/or verification of a valid license.
- Air ambulances - Air ambulance services are regulated by the State when they transport patients out of Colorado. If your air ambulance service agency wants to provide this service, it must be either licensed or authorized by the Colorado Department of Public Health and Environment.
- Complete provider enrollment to become a Health First Colorado EMT provider. Visit the Provider Enrollment web page for enrollment information.
- To be eligible to be reimbursed for Health First Colorado EMT claims, providers must enroll correctly prior to providing services.
Provider Type/Code: 13 - Transportation (Emergency Medical Transportation)- Specialty: Air Ambulance
Specialty Code: 086 - Specialty: County Agency
Specialty Code: 124 - Specialty: Emergency
Specialty Code: 324
- Specialty: Air Ambulance
- To be eligible to be reimbursed for Health First Colorado EMT claims, providers must enroll correctly prior to providing services.
Note: Providers enrolled as any other provider type/code must complete a separate enrollment application to be eligible to provide EMT services.
Non-Emergent Medical Transportation (NEMT) Ambulance Providers
Ambulance providers must complete a separate enrollment application to be eligible to provide Non-Emergent Medical Transportation (NEMT) services.
Payment for Covered Services
Regardless of whether Health First Colorado has actually reimbursed the provider, billing members for covered services is strictly prohibited. Balance billing is prohibited. If reimbursement is made, providers must accept this payment as payment in full (see Program Rule 8.012). The provider may only bill the member for services not covered by Health First Colorado.
Refer to the EMT Regulations in 10 CCR 2505-10 8.018 for detailed coverage and limitations.
Member Eligibility
Emergency Medical Transportation is a benefit for all Health First Colorado members who have a critical or unknown illness or injury that demands immediate medical attention to prevent permanent injury or loss or life. Eligibility for Emergency Medical Transportation services are not limited in the same way as Non-Emergency Medical Transportation (NEMT) services.
Prior Authorization
Prior authorization is not required for ground and air ambulance in emergency situations or for in-state hospital to hospital transport including critical care cases.
All NEMT ambulance requests must be sent to the State Designated Entity (SDE).
Covered Benefits and Limitations
Emergency Medical Transportation (EMT) is a benefit for all Health First Colorado members who have a critical or unknown illness or injury that demands immediate medical attention to prevent permanent injury or loss of life.
Ground Ambulance
The following ground ambulance services are covered:
- Transportation to the closest, most appropriate facility
- Basic or advanced life support that is required during transport
- Critical Care Transportation - facility to facility transport requiring medical care above that offered via non-emergency medical transportation (NEMT)
Air Ambulance
When the point of pick up is inaccessible by a land vehicle or remoteness or other obstacles prohibit transporting the member by land to the nearest appropriate medical facility, the following air ambulance services are covered:
- Basic or advanced life support that is required during transport
- Critical Care Transport - when medically necessary to reach the closest, most appropriate facility Air ambulance providers may bill for air mileage for fixed-wing and rotary-wing aircraft.
Exclusions
The following services are not reimbursable by Health First Colorado:
- Waiting time, cancellations or unapproved additional passengers
- Response calls to emergency locations when no transportation is needed or approved
- Charges when the member is not in the vehicle
- Non-benefit services provided at the scene when transportation is not necessary
- Transportation which is covered by another entity
- Transportation to local treatment programs not enrolled as a Health First Colorado provider
- Transportation of a member who has been pronounced deceased at the time that the ambulance arrives
- Pick up or delivery of prescriptions and/or supplies
- Transportation arranged for a member's convenience when there is no reasonable risk or permanent injury or loss of life
- Transportation to non-emergency medical appointments
Procedure Coding
Health First Colorado uses the Centers for Medicare & Medicaid Services (CMS) Healthcare Common Procedural Coding System (HCPCS). The codes are used for submitting claims for services provided to Health First Colorado members and represent services that may be provided by enrolled, certified Health First Colorado providers.
HCPCS are used to identify and reimburse emergency medical transportation services.
The Department updates and revises HCPCS codes through Health First Colorado billing manuals.
Visit the Provider Rates and Fee Schedule web page for current rates.
Multiple Trips in the Same Day
When billing for one (1) member taking multiple trips in the same day with the same rendering provider, modifier 76 must be used.
When billing for one (1) member taking multiple trips in the same day with different rendering providers, modifier 77 must be used.
Ground Ambulance
| Code | Unit | Description |
|---|---|---|
| A0429 | One Way Trip | Emergency transportation: Ambulance service- Basic Life Support (BLS) |
| A0427 | One Way Trip | Emergency transportation: Ambulance service- Advanced Life Support (ALS), level 1 |
| A0433 | One Way Trip | Ambulance service - Advanced Life Support (ALS), level 2 |
| A0225 | One Way Trip | Emergency transportation: Ambulance service- neonatal transport |
| A0434 | One Way Trip | Specialty care transport (SCT) |
| A0425 | Mile | Ground mileage, per statute mile |
| A0021 | Mile | Ambulance service, outside state per mile, transport |
| A0422 | Per Unit | Ambulance (ALS or BLS) oxygen and oxygen supplies, life-sustaining situation |
Air Ambulance
| Code | Unit | Description |
|---|---|---|
| A0430 | One Way Trip | Ambulance service, conventional air services, transport, one way (fixed wing) |
| A0431 | One Way Trip | Ambulance service, conventional air services, transport, one way (rotary wing) |
| A0435 | Per Mile | Air transport mileage (fixed wing) |
| A0436 | Per Mile | Air transport mileage (rotary wing) |
EMT Billing Information
The 837 Professional (837P) transaction should be utilized for electronic billing.
Claim Type
EMT Claims submitted via the Provider Web Portal are Professional or Professional Crossover Claims.
Diagnosis Codes
The Health First Colorado recognizes the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-10-CM) diagnostic coding reference. See the ICD-10-CM for a full list of diagnosis codes.
Dates of Services
Each detail line includes space to enter two (2) dates of service: a 'From' Date Of Service (FDOS) and a 'To' Date Of Service (TDOS). Both dates must be completed on the electronic record. For services rendered on a single date, complete the FDOS and the TDOS with the same date.
Span Billing
Span billing is not allowed for transportation services.
Place of Service Codes
Use CMS place of service codes. Use place of service codes:
- 41-land transportation
- 42-air transportation
Procedure Codes Each detail line must include a valid EMT procedure code.
EMG (Emergency) Indicator
The Emergency Indicator is used to differentiate some EMT services from Non-Emergent Medical Transportation. A "Y" must be entered to indicate the service was Emergency Medical Transportation. If you leave this field blank, the EMG indicator defaults to Not Sure, indicating the service was Non-Emergent Medical Transportation (NEMT). Failure to enter a Y may result in a claim denial.
Transportation Certification
Complete this field to certify that you have a transportation certificate or trip sheet on file for this service.
Attachments
Beginning 3/1/17, attachments can be submitted with electronic claims submitted via the Provider Web Portal.
CMS 1500 Paper Claim Reference Table
The following paper form reference table shows required, optional and conditional fields and detailed field completion instructions for the EPSDT claim form.
| CMS Field Number and Label | Field is? | Instructions | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Insurance Type | Required | Place an "X" in the box marked as Medicaid. | ||||||||||||
| 1a. Insured's ID Number | Required | Enter the member's Health First Colorado seven (7)-digit Medicaid ID number as it appears on the Health First Colorado Identification card. Example: A123456. | ||||||||||||
| 2. Patient's Name | Required | Enter the member's last name, first name and middle initial. | ||||||||||||
| 3. Patient's Date of Birth/Sex | Required | Enter the member's birth date using two (2) digits for the month, two (2) digits for the date and two (2) digits for the year. Example: 070114 for July 1, 2014. Place an "X" in the appropriate box to indicate the sex of the member. | ||||||||||||
| 4. Insured's Name | Conditional | Complete if the member is covered by a Medicare health insurance policy. Enter the insured's full last name, first name and middle initial. If the insured used a last name suffix (e.g., Jr, Sr), enter it after the last name and before the first name. | ||||||||||||
| 5. Patient's Address | Not Required | |||||||||||||
| 6. Client Relationship to Insured | Conditional | Complete if the member is covered by a commercial health care insurance policy. | ||||||||||||
| 7. Insured's Address | Not Required | |||||||||||||
| 8. Reserved for NUCC Use | Not Required | |||||||||||||
| 9. Other Insured's Name | Conditional | If field 11d is marked "YES", enter the insured's last name, first name and middle initial. | ||||||||||||
| 9a. Other Insured's Policy or Group Number | Conditional | If field 11d is marked "YES", enter the policy or group number. | ||||||||||||
| 9b. Reserved for NUCC Use | ||||||||||||||
| 9c. Reserved for NUCC Use | ||||||||||||||
| 9d. Insurance Plan or Program Name | Conditional | If field 11D is marked "YES", enter the insurance plan or program name. | ||||||||||||
| 10a-c. Is patient's condition related to? | Conditional | When appropriate, place an "X" in the correct box to indicate whether one (1) or more of the services described in field 24 are for a condition or injury that occurred on the job, as a result of an auto accident or other. | ||||||||||||
| 10d. Reserved for Local Use | ||||||||||||||
| 11. Insured's Policy, Group or FECA Number | Conditional | Complete if the member is covered by a Medicare health insurance policy. Enter the insured's policy number as it appears on the ID card. Only complete if field 4 is completed. | ||||||||||||
| 11a. Insured's Date of Birth, Sex | Not Required | Complete if the member is covered by a Medicare health insurance policy. Enter the insured's birth date using two (2) digits for the month, two digits (2) for the date and two (2) digits for the year. Example: 070114 for July 1, 2014. Place an "X" in the appropriate box to indicate the sex of the insured. | ||||||||||||
| 11b. Other Claim ID | Not Required | |||||||||||||
| 11c. Insurance Plan Name or Program Name | Not Required | |||||||||||||
| 11d. Is there another Health Benefit Plan? | Conditional | When appropriate, place an "X" in the correct box. If marked "YES", complete 9, 9a and 9d. | ||||||||||||
| 12. Patient's or Authorized Person's signature | Required | Enter "Signature on File," "SOF" or legal signature. If there is no signature on file, leave blank or enter "No Signature on File." Enter the date the claim form was signed. | ||||||||||||
| 13. Insured's or Authorized Person's Signature | Not Required | |||||||||||||
| 14. Date of Current Illness Injury or Pregnancy | Conditional | Complete if information is known. Enter the date of illness, injury or pregnancy, (date of the last menstrual period) using two (2) digits for the month, two (2) digits for the date and two (2) digits for the year. Example: 070114 for July 1, 2014. Enter the applicable qualifier to identify which date is being reported. 431 - Onset of Current Symptoms or Illness 484 - Last Menstrual Period | ||||||||||||
| 15. Other Date Not | Not Required | |||||||||||||
| 16. Date Patient Unable to Work in Current Occupation | Not Required | |||||||||||||
| 17. Name of Referring Physician | Conditional | |||||||||||||
| 17b. NPI of Referring Physician | Conditional | |||||||||||||
| 18. Hospitalization Dates Related to Current Service | Not Required | |||||||||||||
| 19. Additional Claim Information | Conditional | When applicable, enter the words "TRANSPORT CERT" to certify that you have a transportation certificate or trip sheet on file for this service. | ||||||||||||
| 20. Outside Lab? $ Charges | Not Required | |||||||||||||
| 21. Diagnosis or Nature of Illness or Injury | Required | Enter at least one (1) but no more than 12 diagnosis codes based on the member's diagnosis/condition. Enter applicable ICD-10 indicator. | ||||||||||||
| 22. Medicaid Resubmission Code | Conditional | List the original reference number for resubmitted claims. When resubmitting a claim, enter the appropriate bill frequency code in the left- hand side of the field. 7 - Replacement of prior claim 8 - Void/Cancel of prior claim This field is not intended for use for original claim submissions. | ||||||||||||
| 23. Prior Authorization | Not Required | |||||||||||||
| 24. Claim Line Detail | Information | The paper claim form allows entry of up to six (6) detailed billing lines. Fields 24A through 24J apply to each billed line. Do not enter more than six (6) lines of information on the paper claim. If more than six (6) lines of information are entered, the additional lines will not be entered for processing. Each claim form must be fully completed (totaled). Do not file continuation claims (e.g., Page 1 of 2). | ||||||||||||
| 24A. Dates of Service | Required | The field accommodates the entry of two (2) dates: a "From" date of services and a "To" date of service. Enter the date of service using two (2) digits for the month, two (2) digits for the date and two (2) digits for the year. Example: 010117 for January 1, 2017.
Single Date of Service: Enter the six (6)-digit date of service in the "From" field. | ||||||||||||
| 24B. Place of Service | Required | Enter the Place of Service (POS) code that describes the location where services were rendered. Health First Colorado accepts the CMS place of service codes.
| ||||||||||||
| 24C. EMG | Conditional | Enter a "Y" in the bottom, unshaded area of the field to indicate the service was Emergency Medical Transportation. | ||||||||||||
| 24D. Procedures, Services, or Supplies | Required | Enter the HCPCS procedure code that specifically describes the service for which payment is requested. Only approved codes from the current CPT or HCPCS publications will be accepted. | ||||||||||||
| 24D. Modifier | Not Required | Enter the appropriate procedure-related modifier that applies to the billed service. Up to four (4) modifiers may be entered when using the paper claim form. | ||||||||||||
| 24E. Diagnosis Pointer | Required | Enter the diagnosis code reference letter (A-L) that relates the date of service and the procedures performed to the primary diagnosis. At least one (1) diagnosis code reference letter must be entered. When multiple services are performed, the primary reference letter for each service should be listed first, other applicable services should follow. This field allows for the entry of four (4) characters in the unshaded area. | ||||||||||||
| 24F. $ Charges | Required | Enter the usual and customary charge for the service represented by the procedure code on the detail line. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. Submitted charges cannot be more than charges made to non-Health First Colorado covered individuals for the same service. Do not deduct Health First Colorado co-pay or commercial insurance payments from the usual and customary charges. | ||||||||||||
| 24G. Days or Units | Required | Enter the number of units provided for each procedure code. Enter whole numbers only- do not enter fractions or decimals. | ||||||||||||
| 24H. EPSDT/Family Plan | Not Required | |||||||||||||
| 24I. ID Qualifier | Not Required | |||||||||||||
| 24J. Rendering Provider ID # | Required | In the shaded portion of the field, enter the NPI or Provider ID of the Health First Colorado provider who actually performed or rendered the billed service. This number cannot be assigned to a group or clinic. | ||||||||||||
| 25. Federal Tax ID Number | Not Required | |||||||||||||
| 26. Patient's Account Number | Optional | Enter information that identifies the member or claim in the provider's billing system. Submitted information appears on the Remittance Advice (RA). | ||||||||||||
| 27. Accept Assignment? | Required | The accept assignment indicates that the provider agrees to accept assignment under the terms of the payer's program. | ||||||||||||
| 28. Total Charge | Required | Enter the sum of all charges listed in field 24F. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. | ||||||||||||
| 29. Amount Paid | Conditional | Enter the total amount paid by Medicare or any other commercial health insurance that has made payment on the billed services. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. | ||||||||||||
| 30. Rsvd for NUCC Use | ||||||||||||||
| 31. Signature of Physician or Supplier Including Degrees or Credentials | Required | Each claim must bear the signature of the enrolled provider or the signature of a registered authorized agent. Each claim must have the date the enrolled provider or registered authorized agent signed the claim form. Enter the date the claim was signed using two (2) digits for the month, two (2) digits for the date and two (2) digits for the year. Example: 070116 for July 1, 2016. | ||||||||||||
| 32. 32- Service Facility Location Information 32a- NPI Number 32b- Other ID # | Required | Enter the name, address and ZIP code of the individual or business where the member was seen or service was performed in the following format: 1st Line Name 2nd Line Address 3rd Line City, State and ZIP Code If the Provider Type is not able to obtain an NPI, enter the eight (8)-digit Health First Colorado provider number of the individual or organization. | ||||||||||||
| 33. Billing Provider Info & Ph # | Required | Enter the name of the individual or organization that will receive payment for the billed services in the following format: 1st Line Name 2nd Line Address 3rd Line City, State and ZIP Code | ||||||||||||
| 33a- NPI Number | Required | |||||||||||||
| 33b- Other ID # | If the Provider Type is not able to obtain an NPI, enter the eight (8)-digit Health First Colorado provider number of the individual or organization. | |||||||||||||
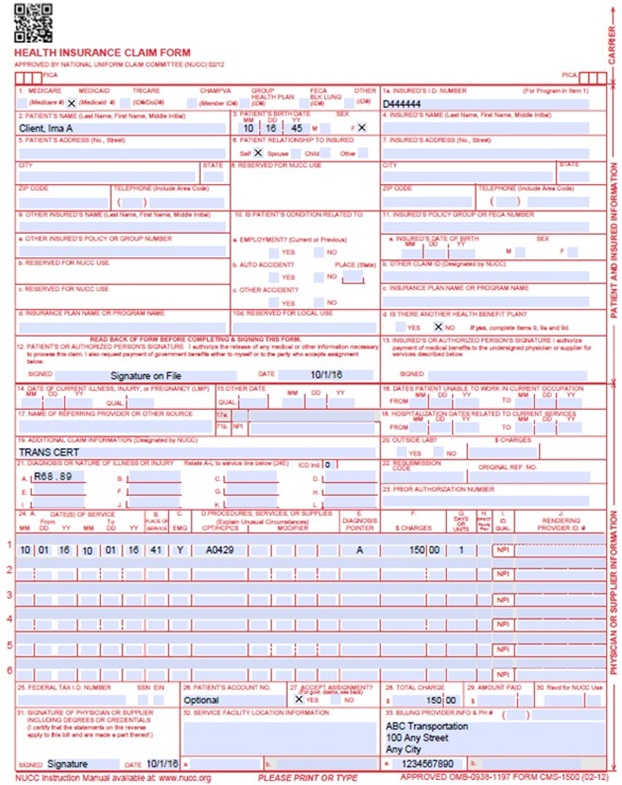
CMS 1500 Transportation Claim Example
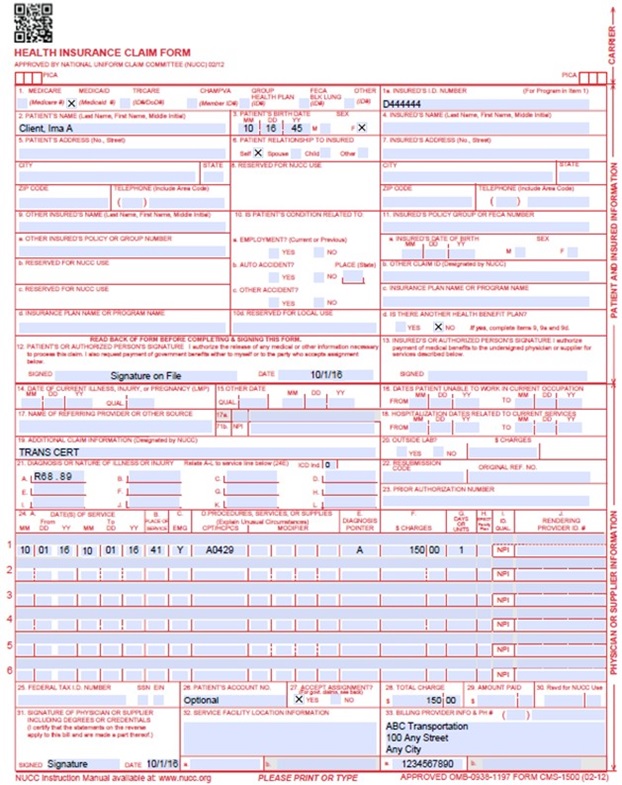
Transportation Third Party Claim - No Mileage Example
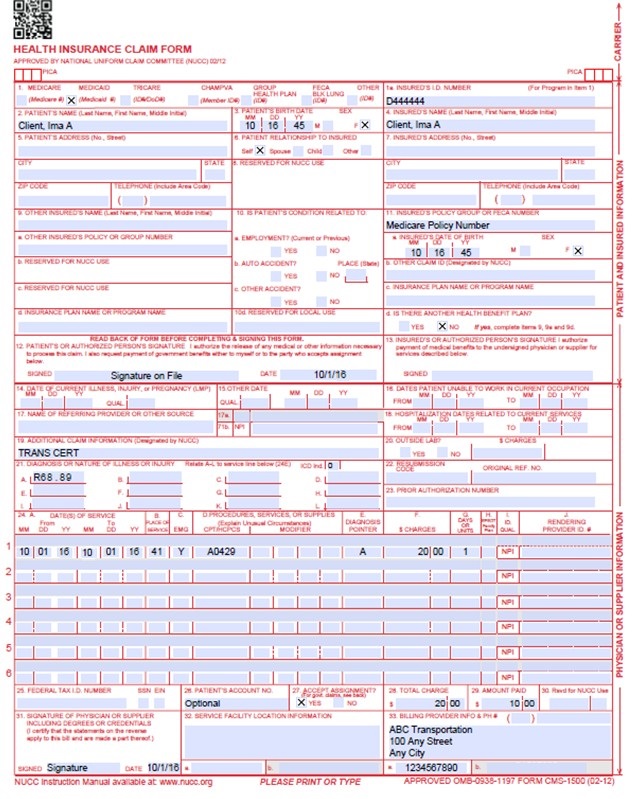
Transportation Crossover Claim Example
Timely Filing
Refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down for more information on timely filing policy, including the resubmission rules for denied claims.
EMT Billing Manual Revisions Log
| Revision Date | Section/Action | Made by |
|---|---|---|
| 12/1/2016 | Manual revised for interChange implementation. For manual revisions prior to 12/01/2016, please refer to Archive. | HPE |
| 12/27/2016 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_2.xlsx | HPE |
| 1/10/2017 | Updates based on Colorado iC Stage Provider Billing Manual Comment Log v0_3.xlsx | HPE |
| 1/19/2017 | Updates based on Colorado iC Stage Provider Billing Manual Comment Log v0_4.xlsx | HPE |
| 1/26/2017 | Updates based on Department 1/20/2017 approval email | HPE |
| 12/12/2017 | Manual revised to separate NEMT and EMT services. Changed the name to EMT Billing Manual. Updates made throughout to align with current policies and billing rules. | HCPF |
| 4/18/2018 | Added clarification that interfacility transportation is an EMT benefit. Clarified EMG Indicator left blank defaults to "Not Sure." | HCPF |
| 6/22/2018 | Updated billing info and timely filing to point to General Billing Manual | HCPF |
| 12/21/2018 | Clarification to signature requirements | HCPF |
| 3/18/2019 | Clarification to signature requirements | HCPF |
| 12/12/2019 | Added two lines for the proc codes, one line about mileage, and an explanation that EMT does not have the same eligibility restrictions as NEMT | HCPF |
| 12/27/2019 | Converted to web page | HCPF |
| 9/14/2020 | Added Line to Box 32 under the CMS 1500 Paper Claim Reference Table | HCPF |
| 7/22/2021 | Added verbiage for multiple trips in same day for same member | HCPF |