Dialysis Billing Manual
- Dialysis
- Billing Information
- Dialysis Benefits
- Reimbursement
- UB-04 Paper Claim Reference Table
- Timely Filing
- Institutional Provider Certification
- Dialysis Revisions Log
Return to Billing Manuals Web Page
Dialysis
Providers must be enrolled as a Health First Colorado (Colorado's Medicaid program) provider in order to:
- Treat a Health First Colorado member
- Submit claims for payment to Health First Colorado
Health First Colorado provides hemodialysis and peritoneal dialysis benefits to eligible members in outpatient, state-approved freestanding dialysis treatment centers and the home setting. These services are billed on the UB-04 institutional paper claim form or as an 837 Institutional (837I) electronic transaction.
State-approved non-routine services provided outside of the routine dialysis treatment should be billed and reimbursed separately. The services must be billed on the CMS 1500 professional paper claim form or as an 837 Professional (837P) electronic transaction using the dialysis center National Provider Identifier (NPI) number.
Providers should refer to the Code of Colorado Regulations, Program Rules (10 C.C.R. 2505-10 8.310), for specific information when providing dialysis services.
Dialysis may be provided as part of inpatient hospital treatment and included in the hospital inpatient claim. Refer to the Dialysis Benefits section below.
Billing Information
Refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down menu for general billing information.
Dialysis Benefits
Inpatient Hospital:
Inpatient hemodialysis is a benefit when:
- Hospitalization is required for an acute medical condition requiring hemodialysis treatment.
- Hospitalization is required for a covered medical condition and the member receives regular maintenance outpatient hemodialysis treatment.
- Hospitalization is required for placement or repair of the hemodialysis route (shunt or cannula).
- Inpatient hemodialysis payment is included as part of the Diagnosis Related Group (DRG).
Hospital admissions solely for hemodialysis are not a Health First Colorado benefit.
Outpatient: State-Approved Dialysis Treatment Center
A dialysis treatment center is an independent, free-standing center or a department of a licensed hospital enrolled as a dialysis center that is planned, organized, operated and maintained to provide outpatient hemodialysis treatment and/or training for home use of hemodialysis or peritoneal equipment. Other conditions for participation are those specifically entered into the agreement with the Department of Health Care Policy & Financing (the Department).
Continued outpatient hemodialysis is a benefit when:
- Training of the eligible recipient to perform self-treatment in the home environment is contraindicated.
- The eligible member is not a proper candidate for self-treatment in a home environment.
- The home environment of the eligible member contraindicates self-treatment.
- The eligible member is awaiting a kidney transplant.
Home Dialysis
The high costs of dialysis treatments and the budgetary limitations of Health First Colorado require that all members be considered for the most cost-efficient method of dialysis based upon their individual medical diagnosis and condition. Such treatments include home hemodialysis and peritoneal dialysis.
The participating dialysis center shall be responsible for the provision and maintenance of all equipment and necessary fixtures required for home dialysis and the provision of all supplies.
All eligible members approved for self-treatment must be trained in the use of hemodialysis or peritoneal equipment while undergoing outpatient treatments.
Training must be provided by qualified personnel of a hospital with a separate dialysis center or by qualified personnel of an independent, free-standing dialysis treatment center.
The participating dialysis center must provide and install quality hemodialysis equipment or peritoneal equipment to be used by the member at home and must provide routine medical surveillance of the member's adaptation and adjustment to the self-treatment.
Any facility providing regularly scheduled outpatient dialysis treatments or billing for supplies necessary to perform the various types of home dialysis treatments shall apply for a separate Health First Colorado Provider ID. Such provider shall be designated solely for the purpose of claims submission for dialysis services.
For appropriate reimbursement, Condition Code 74 must be used on home dialysis claims.
Emergency Medicaid and End-Stage Renal Disease
Effective February 1, 2019, End-Stage Renal Disease (ESRD) is considered an emergency medical condition for purposes of coverage under EMS. Recipients of EMS can receive care and services related to the treatment of ESRD, including but not limited to scheduled dialysis at a free-standing facility, home dialysis, and vascular access procedures.
An emergency medical condition is defined as "a medical condition (including emergency labor and delivery) manifesting itself by acute symptoms of sufficient severity (including severe pain) such that the absence of immediate medical attention could reasonably be expected to result in:
- Placing the patient's health in serious jeopardy
- Serious impairment to bodily function
- Serious dysfunction of any bodily organ or party"42 U.S.C. § 1396b(v)(3), Colorado Revised Statutes § 24-76.5-102(1)
Recipients of Emergency Medicaid Services can receive care and services related to the treatment of ESRD at independent, free-standing dialysis centers.
Benefits for vascular access procedures and pre-surgery imaging are considered to be necessary in the treatment of ESRD.
Dialysis is not a covered benefit in the outpatient hospital setting.
As of January 1, 2022, home dialysis is a covered benefit for recipients of Emergency Medicaid.
Refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down for emergency services billing guidance.
Reimbursement
The amount of payment for outpatient dialysis or necessary supplies for home dialysis treatments, when provided by a separate dialysis center within a hospital or an independent, free-standing dialysis treatment center approved for participation by the Department, shall be the lesser of the dialysis center's charges or the currently posted Health First Colorado rate.
The following dialysis services are reimbursed at the lower of the composite Medicare rate ceiling or the individual center's Medicare facility rate:
- Outpatient hemodialysis
- Outpatient peritoneal dialysis
- Continuous Ambulatory Peritoneal Dialysis (CAPD)
- Continuous Cycling Peritoneal Dialysis (CCPD)
There is no reimbursement for home dialysis, except for necessary home dialysis equipment and supplies.
Routine Services
Routine services performed with the dialysis treatment shall be considered part of the composite rate and billed on the UB-04 claim form or electronically on the 837I transaction.
Report routine services with appropriate revenue codes. Refer to Appendix Q on the Billing Manuals web page under the Appendices drop-down for valid dialysis revenue codes.
Charges by a dialysis facility for routine drugs and laboratory services, electrocardiograms (EKGs) and X-rays are considered part of the dialysis treatment.
Non-Routine Services
Non-routine services performed in addition to the dialysis treatment shall be reimbursed separately and billed on the CMS 1500 professional claim form or electronically as an 837P transaction. This requires that the provider use the appropriate Healthcare Common Procedure Coding System (HCPCS) codes designated for the service provided. Only non-routine services performed in addition to the dialysis treatment may be included on the professional claim.
The amount of payment for non-routine outpatient dialysis treatments, when provided by a separate dialysis center within a hospital or an independent, free-standing dialysis treatment center, shall be based upon the Health First Colorado fee schedule.
- Non-routine drugs must be billed on the CMS 1500 professional paper claim form or as an 837 Professional (837P) electronic transaction using the dialysis center NPI number.
- Drugs not dispensed by the dialysis provider are billed by and reimbursed to the dispensing pharmacy.
- Physician's charges for EKG or X-ray services must be billed by the physician.
- A physician must supervise the process when blood is furnished and may bill for any professionally rendered covered service using their NPI number.
Laboratory Services
- Routine laboratory services are included as part of the dialysis service reimbursement.
- Non-routine laboratory services are reimbursed as laboratory services separate from the dialysis treatment. Hospitals having separate dialysis units must submit services according to outpatient hospital laboratory regulations and UB-04 institutional billing instructions.
- A freestanding dialysis center that performs its own laboratory tests must be licensed as an independent clinical laboratory and enrolled in Health First Colorado as an independent laboratory. The non-routine laboratory services must be billed under the independent laboratory's NPI number on the CMS 1500 professional claim form or electronically as an 837P transaction.
- If an outside laboratory provides the service, that laboratory must bill for the service. All routine laboratory services performed by a dialysis treatment facility, with the designation as a certified clinical laboratory, or as a certified independent laboratory are included as part of the dialysis treatment reimbursement. All routine tests must be performed by the facility, with designation as a certified clinical laboratory, and reimbursed as part of the composite rate or performed by a certified independent outside laboratory and billed to the facility performing the dialysis treatment.
The following procedures and drugs constitute routine services. These services are included as part of the dialysis center’s composite rate.
| Routine Labs / Procedures | ||
| Alkaline Phosphatase | All Hematocrit and Clotting time tests | Aspartate Aminotransferase (AST) or Serum Glutamic-Oxaloacetic Transaminase |
| Assay of Parathormone | Automated battery of tests (SMA-12) | Bicarbonate Dialysate |
| Blood Urea Nitrogen (BUN) | Complete Blood Count (CBC) | Carbon Dioxide (CO2) |
| Dialysate Protein | Electrolyte panel | Hematocrit |
| Hemoglobin | Hepatic function panel | Iron |
| Lactate Dehydrogenase (LDH) | Magnesium | Metabolic panel |
| Platelet Count | Red Blood Count | Renal function panel |
| Reticulocyte | Saline Flush | Serum Albumin |
| Serum Aluminum | Serum Bicarbonate | Serum Calcium |
| Serum Chloride | Serum Creatinine | Serum Ferritin |
| Serum Phosphorous | Serum Potassium | Serum Sodium |
| Specimen Collection | Total Protein | Transferrin |
| Vitamin D | White Blood Count | |
| Routine Drugs | ||
| Calcitriol | Darbepoetin alfa, Epoetin alfa, or Epogen | Doxercalciferol |
| Hematinics | Heparin | Iron dextran, Iron sucrose, Sodium ferric gluconate complex in sucrose injection, or Ferumoxytol |
| Oxygen | Paricalcitol | Parsabiv (etelcalcetide) |
Nonparenteral items may not be billed separately by the dialysis center but may be billed directly to Health First Colorado by the supplier. Nonparenteral items administered during the dialysis treatment are reimbursed as part of the composite rate.
UB-04 Paper Claim Reference Table
The information in the following table provides instructions for completing form locators as they appear on the paper UB-04 claim form. Instructions for completing the UB-04 institutional claim form are based on the current National Uniform Billing Committee (NUBC) UB-04 Reference Manual. Unless otherwise noted, all data form locators on the UB-04 have the same attributes (specifications) for Health First Colorado as those indicated in the NUBC UB-04 Reference Manual.
All code values listed in the NUBC UB-04 Reference Manual for each form locator may not be used for submitting paper claims to Health First Colorado. The appropriate code values listed in this manual must be used when billing Health First Colorado.
The UB-04 Certification document must be completed and attached to all claims submitted on the paper UB-04. Completed UB-04 paper Health First Colorado claims, including hardcopy Medicare claims, should be mailed to the correct fiscal agent address listed in Appendix A located on the Billing Manuals web page under the Appendices drop-down.
Do not submit "continuation" claims. Each claim form has a set number of billing lines available for completion. Do not crowd more lines on the form.
Billing lines in excess of the designated number are not processed or acknowledged. Claims with more than one (1) page may be submitted through the Provider Web Portal.
Bill with a date span (From and To dates of service) only if the service was provided every consecutive day within the span. The From and To dates must be in the same month.
The Paper Claim Reference Table below lists the required, optional and conditional form locators for submitting the paper UB-04 claim form to Health First Colorado.
| Form Locator and Labels | Completion Format | Instructions | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Billing Provider Name, Address, Telephone Number | Text | Required
Abbreviate the state using standard post office abbreviations. Enter the telephone number. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2. Pay-to Name, Address, City, State | Text | Required only if different from form locator 1.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3a. Patient Control Number | Up to 20 characters: Letters, numbers or hyphens | Optional Enter information that identifies the member or claim in the provider's billing system. Submitted information appears on the Remittance Advice (RA). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3b. Medical Record Number | 17 digits | Optional Enter the number assigned to the member to assist in retrieval of medical records. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4. Type of Bill | 3 digits | Required
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5. Federal Tax Number | None | Submitted information is not entered into the claim processing system. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 6. Statement covers period From/Through | From:6 digits MMDDYY Through: 6 digits MMDDYY | Required This form locator must reflect the beginning and ending dates of service. When span billing for multiple dates of service and multiple procedures, complete form locator 45 (Service Date). Providers not wishing to span bill following these guidelines must submit one (1) claim per date of service. "From" and "Through" dates must be the same. All line-item entries must represent the same date of service. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 8a. Patient Identifier | Text | Submitted information is not entered into the claim processing system. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 8b. Patient Name | Up to 25 characters, letters and spaces | Required Enter the member's last name, first name and middle initial. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9a. Patient Address - Street | Characters letters and numbers | Required Enter the member's street/post office box as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9b. Patient Address - City | Text | Required Enter the member's city as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9c. Patient Address - State | Text | Required Enter the member's state as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9d. Patient Address - ZIP | Digits | Required Enter the member's zip code as determined at the time of admission. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9e. Patient Address - Country Code | Digits | Optional | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 10. Birthdate | 8 digits (MMDDCCYY) | Required Enter the member's birthdate using two (2) digits for the month, two (2) digits for the date, and four (4) digits for the year (MMDDCCYY format). Example: 01012010 for January 1, 2010 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 11. Patient Sex | 1 letter | Required Enter an M (male) or F (female) to indicate the member's sex. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 12. Admission Date | 6 digits | Not Required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 13. Admission Hour | 6 digits | Not required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 14. Admission Type | 1 digit | Not Required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 15. Source of Admission | 1 digit | Required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 16. Discharge Hour | 2 digits | Not Required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 17. Patient Discharge Status | 2 digits | Required Dialysis must use code 01. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 18-28. Conditions Codes | 2 digits | Conditional Complete with as many codes necessary to identify conditions related to this bill. Condition Codes 06 ESRD member - First 18 months entitlement Renal dialysis settings 71 Full care unit 72 Self-care unit 73 Self-care training 74 Home care 75 Home care - 100 percent reimbursement | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 29. Accident State | 2 digits | Optional | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 31 - 34. Occurrence Code/Date | 2 digits and 6 digits | Conditional
*Other Payer occurrence codes 24 and 25 must be used when applicable. The claim must be submitted with the third-party information | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 35-36. Occurrence Span Code From/ Through | Digits | Leave blank | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 38. Responsible Party Name/Address | None | Leave blank | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 39-41. Value Codes and Amounts | 2 characters and up to 9 digits | Conditional
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 42. Revenue Code | 4 digits | Required Enter the revenue code that identifies the specific service provided. List revenue codes in ascending order. Refer to Appendix Q on the Billing Manuals web page under the Appendices drop-down for valid dialysis revenue codes. A revenue code must appear only once per date of service. * If more than one (1) of the same services is provided on the same day, combine the units and charges on one (1) line accordingly. Complete with as many codes as necessary to identify conditions related to this bill. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 43. Revenue Code Description | Text | Required
Example:
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 44.HCPCS/Rates/Health Insurance Prospective Payment System (HIPPS) Rate Codes | 5 digits | Conditional
HCPCS codes cannot be repeated for the same date of service. Combine the units in form locator 46 (Units) to report multiple services. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 45. Service Date | 6 digits | For span bills only: Enter the date of service using MMDDYY format for each detail line completed. Each date of service must fall within the date span entered in the "Statement Covers Period" field (form locator 6). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 46. Service Units | 3 digits | Required Enter a unit value on each line completed. Use whole numbers only. Do not enter fractions or decimals and do not show a decimal point followed by a 0 to designate whole numbers (e.g., Do not enter 1.0 to signify one [1] unit). For span bills, the units of service reflect only those visits, miles or treatments provided on dates of service in form locator 45. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 47. Total Charges | 9 digits | Required Enter the total charge for each line item. Calculate the total charge as the number of units multiplied by the unit charge. Do not subtract Medicare or third-party payments from line charge entries. Do not enter negative amounts. A grand total on line 23 is required for all charges. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 48. Non-covered Charges | Up to 9 digits | Conditional Enter incurred charges that are not payable by Health First Colorado. Non-covered charges must be entered in both form locator 47 (Total Charges) and form locator 48 (Non-Covered Charges). Each column requires a grand total on line 23. Non-covered charges cannot be billed for outpatient hospital laboratory or hospital-based transportation services. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 50. Payer Name | 1 letter and text | Required
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 51. Health Plan ID | 10 digits | Required Enter the NPI number assigned to the billing provider. Payment is made to the enrolled provider or agency that is assigned this number. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 52. Release of Information | N/A | Submitted information is not entered into the claim processing system. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 53. Assignment of Benefits | N/A | Submitted information is not entered into the claim processing system. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 54. Prior Payments | Up to 9 digits | Conditional Complete when there are Medicare or third-party payments. Enter third party and/or Medicare payments. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 55. Estimated Amount Due | Up to 9 digits | Conditional Complete when there are Medicare or third-party payments. Enter the net amount due from Health First Colorado after provider has received other third party, Medicare or member liability amount. Medicare Crossovers Enter the sum of the Medicare coinsurance plus Medicare deductible less third-party payments and member payments. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 56. National Provider Identifier (NPI) | 10 digits | Required Enter the billing provider's 10-digit National Provider Identifier (NPI). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 57. Other Provider ID | Optional Submitted information is not entered into the claim processing system. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 58. Insured's Name | Up to 30 characters | Required Enter the member's name on the Health First Colorado line. Other Insurance/Medicare Complete additional lines when there is third party coverage. Enter the policyholder's last name, first name and middle initial. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 60. Insured's Unique ID | Up to 20 characters | Required Enter the insured's unique identification number assigned by the payer organization exactly as it appears on the health insurance card. Include letter prefixes or suffixes shown on the card. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 61. Insurance Group Name | 14 letters | Conditional Complete when there is third party coverage. Enter the name of the group or plan providing the insurance to the insured exactly as it appears on the health insurance card. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 62. Insurance Group Number | 17 digits | Conditional Complete when there is third party coverage. Enter the identification number, control number or code assigned by the carrier or fund administrator identifying the group under which the individual is carried. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 63. Treatment Authorization Code | Up to 18 characters | Conditional Complete when the service requires a Prior Authorization Request (PAR). Enter the authorization number in this form locator if a PAR is required and has been approved for services. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 64. Document Control Number | none | Conditional | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 65. Employer Name | Text | Conditional Complete when there is third party coverage. Enter the name of the employer that provides health care coverage for the individual identified in form locator 58 (Insured Name). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 66. Diagnosis Version Qualifier | Submitted information is not entered into the claim processing system. Enter applicable International Classification of Diseases (ICD) indicator to identify which version of ICD codes is being reported. 0ICD-10-CM (DOS 10/1/15 and after) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 67. Principal Diagnosis Code | Up to 6 digits | Not required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 67A. - 67Q. - Other Diagnosis | 6 digits | Optional Enter the exact diagnosis code corresponding to additional conditions that co-exist at the time of admission or develop subsequently and which effect the treatment received or the length of stay. Do not add extra zeros to the diagnosis code. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 69. Admitting Diagnosis Code | 6 digits | Not required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 70. Patient Reason Diagnosis | Submitted information is not entered into the claim processing system. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 71. PPS Code | Submitted information is not entered into the claim processing system. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 72. External Cause of Injury code (E-Code) | 6 digits | Optional Enter the diagnosis code for the external cause of an injury, poisoning or adverse effect. This code must begin with an "E." | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 74. Principal Procedure Code/Date | 7 characters and 6 digits | Conditional Enter the ICD-10-CM procedure code for the principal procedure performed during this billing period and the date on which procedure was performed. Enter the date using MMDDYY format. Apply the following criteria to determine the principal procedure: The principal procedure is not performed for diagnostic or exploratory purposes. This code is related to definitive treatment. The principal procedure is most related to the primary diagnosis. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 74A. Other Procedure Code/Date | 7 characters and 6 digits | Conditional Complete when there are additional significant procedure codes. Enter the procedure codes identifying all significant procedures other than the principal procedure and the dates on which the procedures were performed. Report those that are most important for the episode of care and specifically any therapeutic procedures closely related to the principal diagnosis. Enter the date using MMDDYY format. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 76. Attending NPI - Required | NPI - 10 digits | Health First Colorado ID Required NPI - Enter the 10-digit NPI number assigned to the physician having primary responsibility for the member's medical care and treatment. This number is obtained from the physician and cannot be a clinic or group number. (If the attending physician is not enrolled in Health First Colorado, or if the member leaves the ER before being seen by a physician, the hospital may enter their individual numbers.) Hospitals and FQHCs may enter the member's regular physician's 10- digit NPI in the Attending Physician ID form locator if the locum tenens physician is not enrolled in Health First Colorado. QUAL - Enter "1D" for Health First Colorado Enter the attending physician's last and first name. This form locator must be completed for all services. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 77. Operating NPI | Not required Submitted information is not entered into the claim processing system. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 78 - 79. Other ID | NPI - 10 digits | Conditional Complete when attending physician is not the Primary Care Provider (PCP) or to identify additional physicians. Ordering, Prescribing, or Referring Provider NPI - when applicable NPI - Enter up to two (2) 10-digit NPI numbers when applicable. This form locator identifies physicians other than the attending physician. If the attending physician is not the PCP or if a clinic is a PCP agent, enter the PCP NPI number as the referring physician. The name of the Health First Colorado member's PCP appears on the eligibility verification. Review either for eligibility or PCP. Health First Colorado does not require that the PCP number appear more than once on each claim submitted. The attending physician's last and first name are optional. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 80. Remarks | Text | Enter specific additional information necessary to process the claim or fulfill reporting requirements. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 81. Code - QUAL/CODE/VALUE (a-d) | Qualifier: 2 digits Taxonomy Code: 10 digits | Optional Complete both the qualifier and the taxonomy code for the billing provider in field 81CC-a. Field 81CC-a must be billed with qualifier B3 for the taxonomy code to be captured in the claims processing system. If B3 is missing, no taxonomy code will be captured in the claims processing system. Only one (1) taxonomy code can be captured from field 81CC. If more than one (1) taxonomy code is provided, only the first instance of B3 and taxonomy code will be captured in the claims processing system. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
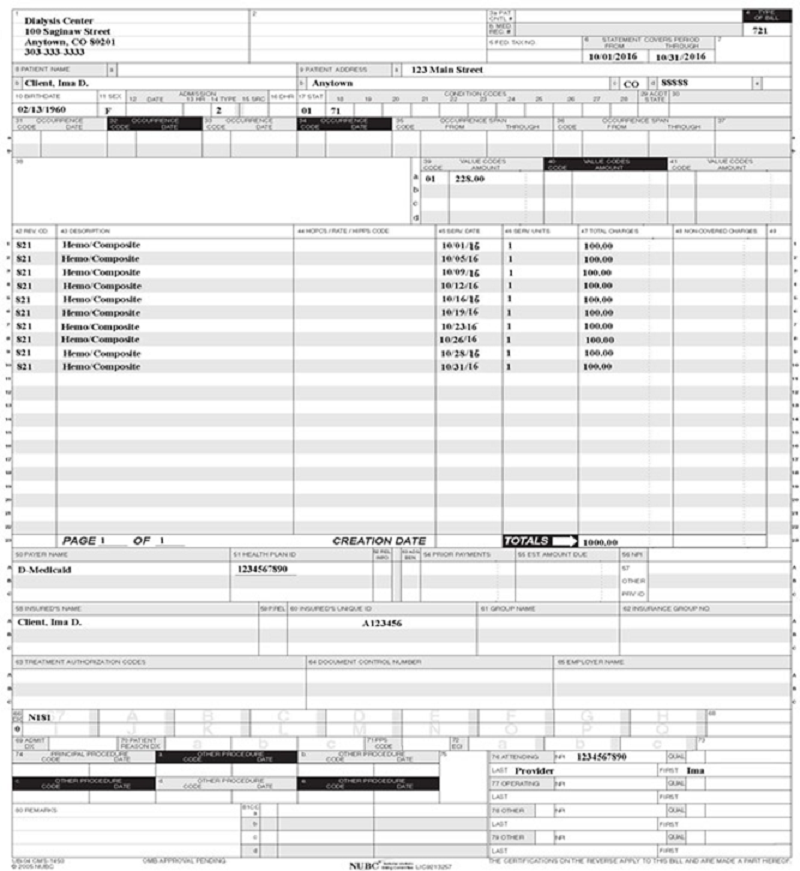
Dialysis UB-04 Claim Example
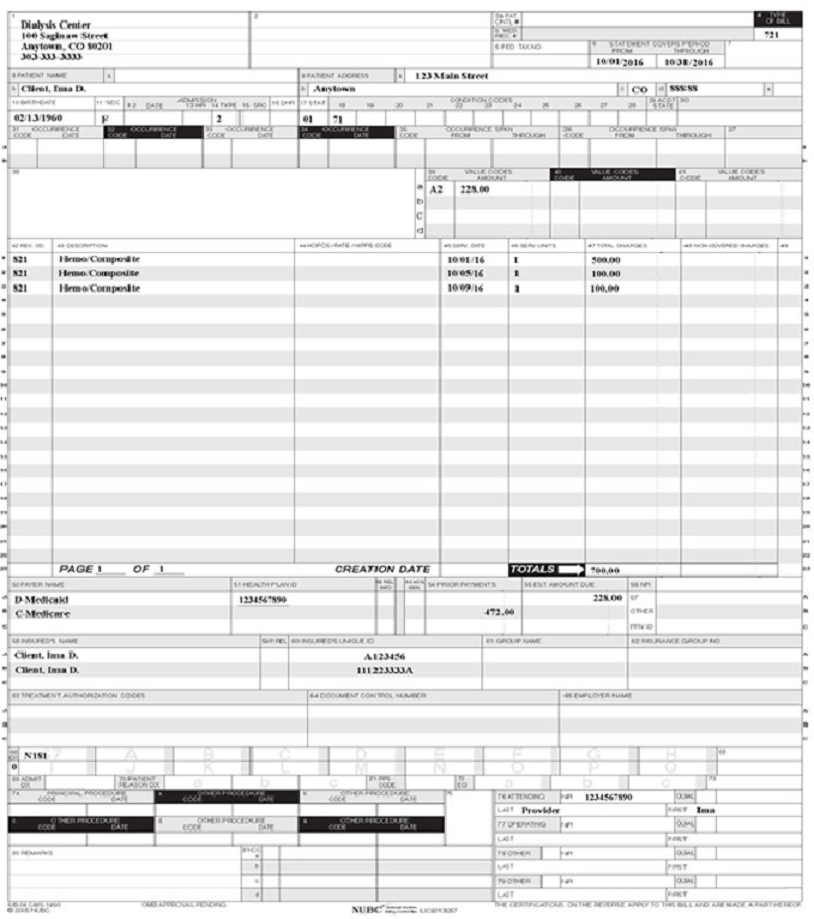
Dialysis UB-04 Crossover Claim Example
Timely Filing
Refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down for more information on timely filing policy, including the resubmission rules for denied claims.
Institutional Provider Certification
The Institutional Provider Certification form is available on the Provider Forms web page under the Claim Forms and Attachments drop-down menu.
Dialysis Revisions Log
| Revision Date | Section/Action | Made by |
|---|---|---|
| 12/1/2016 | Manual revised for interChange implementation. For manual revisions prior to 12/01/2016, please refer to Archive. | HPE (now DXC) |
| 12/27/2016 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_2.xlsx | HPE (now DXC) |
| 1/10/2017 | Updates based on Colorado iC Stage Provider Billing Manual Comment Log v0_3.xlsx | HPE (now DXC) |
| 1/19/2017 | Updates based on Colorado iC Stage Provider Billing Manual Comment Log v0_4.xlsx | HPE (now DXC) |
| 1/26/2017 | Updates based on Department 1/20/2017 approval email | HPE (now DXC) |
| 3/13/2017 | Updated the Type of Bill section in the Paper Claims Table to reflect the NUBC manual | HCPF |
| 5/26/2017 | Updates based on Fiscal Agent name change from HPE to DXC | DXC |
| 1/2/2018 | Revenue Code Submission Update - instructions for reporting an NDC | DXC |
| 6/25/2018 | Updated billing and timely to point to general manual | HCPF |
| 6/28/2018 | Minor formatting edit | HCPF |
| 1/22/2019 | Many updates and clarifications were made throughout the billing manual. A section about "Emergency Medicaid & End-Stage Renal Disease" was added. The list of routine labs, procedures, and drugs was expanded. | HCPF |
| 6/17/2019 | Updated Appendices' links and verbiage | DXC |
| 12/10/2019 | Converted to web page | HCPF |
| 8/7/2020 | Updated item 81 of the Paper Claim Reference Table for taxonomy code billing | DXC |
| 7/15/2021 | Updated link for more ESRD emergency services information | HCPF |
| 12/1/2021 | Updated EMS ESRD to include home dialysis as of Jan. 1, 2022 Added condition code 74 language for home dialysis. | HCPF |
| 5/11/2022 | Updated routine and nonroutine section for clarity | HCPF |
| 9/19/2023 | Updated EMS ESRD to include vascular access procedures and pre-surgery imaging and made some minor edits for consistency | HCPF |
| 1/26/2024 | Added clarifying language under Emergency Medicaid and End-Stage Renal Disease | HCPF |
| 8/19/2025 | Added Value Code D6 to UB-04 Paper Claim Reference Table | HCPF |