Colorado Choice Transitions (CCT) Program Reference Manual
- Program Overview
- Policy Guidance for Services
- Prior Authorization Requests (PARs) for CCT
- PAR Submission
- PAR Form Instructional Reference Table
- Claim Submission
- Paper Claim Reference Table
- CCT Procedure Code Table
- CCT- BI Services Procedure Code Table (Special Program Code 95)
- CCT- EBD 65+ Services Procedure Code Table (Special Program Code 95)
- CCT- EBD 18- 64 Services Procedure Code Table (Special Program Code 95)
- CCT- CMHS Services Procedure Code Table (Special Program Code 95)
- CCT- DD Services Procedure Code Table (Special Program Code 95)
- CCT- SLS Services Procedure Code Table (Special Program Code 95)
- CCT Claim Examples
- Timely Filing
- Colorado Choice Transitions Program Revision Log
Return to Billing Manuals Web Page
Program Overview
Colorado Choice Transitions (CCT), part of the federal Money Follows the Person Rebalancing Demonstration, is a five-year grant program. The primary goal is facilitating the transition of Health First Colorado (Colorado's Medicaid Program) members from nursing and other long-term care (LTC) facilities to the community using home and community based (HCBS) services and supports. Services are intended to promote independence, improve the transition process, and support individuals in the community. Participants of the CCT program will have access to qualified waiver services as well as demonstration services. They will be enrolled in the program for up to 365 days after which time they will enroll into one of five HCBS waivers so long as they remain Medicaid eligible. Days in a hospital or LTC facility for a period of less than 30 days during the enrollment period will not count towards the 365 days. Qualified services are HCBS waiver services that will continue once the CCT program has ended if the member continues to be eligible for HCBS. Demonstration services are enhanced services provided during an individual's enrollment in the demonstration program post-transition and end on the last day of CCT enrollment. The grant funding will also be used to streamline and improve the HCBS systems in Colorado.
Health First Colorado members participating in CCT must meet long-term care Health First Colorado eligibility requirements (which include functional and financial eligibility), reside in a long-term care facility for a period of no less than ninety days (90) not counting days for rehabilitation, have been Medicaid eligible for one day, and be willing to move to qualified housing as defined in federal statute. To participate, members must meet financial, medical, and program criteria to access services through the CCT program and be willing to receive services in their homes or communities. A member who receives services through the CCT program is also eligible for all Health First Colorado State Plan services. When a member chooses to receive services under a waiver and the CCT program, the services must be provided by certified Health First Colorado providers.
The CCT program will complement the Elderly, Blind, and Disabled Waiver, Persons with Brain Injury Waiver, Community Mental Health Supports Waiver, Persons with Developmental Disabilities Wavier, and Supported Living Services Waiver. The populations that will be transitioned through the program include: elderly adults aged 65 years or older residing in Health First Colorado nursing facilities, adults aged 18-64 with physical disabilities residing in Health First Colorado nursing facilities, adults aged 18 and older with developmental disabilities residing in Intermediate Care Facilities (ICFs) and Health First Colorado nursing facilities, and adults 65 years and older and individuals under 22 residing in institutions for mental disease (IMDs).
Note: The Department of Health Care Policy & Financing (the Department) periodically modifies billing information. Therefore, the information in this manual is subject to change, and the manual is updated as new billing information is implemented.
Policy Guidance for Services
The Services and Supports Desk Reference offers essential information on CCT demonstration services to providers, members, and stakeholders. The information includes service definitions, minimum provider qualifications, service rates, and other pertinent information. The Department may periodically modify policy guidance.
Providers are notified of changes in policy guidance in the monthly HCBS Provider Bulletin and other Department communications.
Prior Authorization Requests (PARs) for CCT
All CCT services require prior approval before they can be reimbursed by the Health First Colorado. Case management agencies (CMA) complete the Prior Authorization Request for CCT according to instructions provided by the Department.
The case management agencies responsibilities include, but are not limited to:
- Assessing needs,
- Determining CCT program eligibility,
- Service planning and authorization,
- Care coordination,
- Risk mitigation,
- Service monitoring,
- Monitoring the health, welfare and safety of the member,
- Promotion of member's self-advocacy, and
- Coordination of the member's transition from the CCT program to one of the existing HCBS waivers at the end of the member's participation on the CCT program, as long as the member remains eligible.
PAR Submission
All CCT PAR forms are filed via the "Bridge" which directly interfaces with the Colorado interChange System. Access to the Bridge is accomplished via the Medicaid Enterprise User Provisioning System (MEUPS).
Consumer Directed Attendant Support Services (CDASS)
For members authorized to receive CDASS, case managers will need to enter the data into the web portal maintained by Financial Management Service Provider (FMS) in addition to sending a PAR to the Department.
Case managers may also use the PAR form maintained by FMS to create the entire PAR for a member receiving CDASS as a part of the CCT program. In addition, case managers will need to fax the final PAR approval letter to FMS before attendant timesheets will be paid.
PAR Form Instructional Reference Table
| Field Label | Completion Format | Instructions |
| PA Number being revised | Conditional Complete if PAR is a revision. Indicate original PAR number assigned. |
|
| Revision | Check box Yes No |
Required Check the appropriate box. |
| Client Name | Text | Required Enter the member's last name, first name, and middle initial. Example: Adams, Mary A. |
| Client ID | 7 characters, a letter prefix followed by six numbers | Required Enter the member's state identification number. This number consists of a letter prefix followed by six numbers. Example: A123456 |
| Sex | Check box M F |
Required Check the appropriate box. |
| Birthdate | 6 numbers (MM/DD/YY) |
Required Enter the member's birth date using MM/DD/YY format. Example: January 1, 2010 = 01/01/10. |
| Date of Discharge | 6 numbers (MM/DD/YY) |
Required Enter the member's date of discharge from qualified facility. |
| Requesting Physician Provider # | 8 numbers | Required Enter the eight-digit Health First Colorado provider number of the requesting provider. |
| Client's County | Text | Required Enter the member's county of residence. |
| Case Number (Agency Use) | Text | Optional Enter up to twelve characters, (numbers, letters, and hyphens), which help identify the claim or member. |
| Dates Covered (From/Through) |
6 numbers for from date and 6 numbers for through date (MM/DD/YY) |
Required Enter PAR start date and PAR end date. |
| Qualified/Demonstration Services Description | Text | N/A List of approved procedure codes for qualified and demonstration services. |
| Modifier | 2 Letters | Required +The alphanumeric values in this column are standard and static and cannot be changed. |
| Max # Units | Number | Required Enter the number of units next to the services being requested for reimbursement. |
| Cost Per Unit | Dollar Amount | Required Enter cost per unit of service. |
| Total $ Authorized | Dollar Amount | Required The dollar amount authorized for this service automatically populates. |
| Comments | Text | Optional Enter any additional useful information. For example, if a service is authorized for different dates than in Dates Covered field, please include the HCPCS procedure code and date span here. |
| Total Authorized CCT Qualified Service Expenditures | Dollar Amount | Required Total automatically populates. |
| Total Authorized CCT Demonstration Service Expenditures | Dollar Amount | Required Total automatically populates. |
| Grand Total of CCT Qualified and Demonstration Services | Dollar Amount | Required Total automatically populates. |
| Plus Total Authorized Home Health Expenditures (Sum of Authorized Home Health Services during the HCBS Care Plan Period) |
Dollar Amount | Required Enter the total Authorized Home Health expenditures. |
| Equals Client's Maximum Authorized Cost | Dollar Amount | Required The sum of CCT Expenditures + Home Health Expenditures automatically populates. |
| Number of Days Covered | Number | Required The number of days covered automatically populates. |
| Average Cost Per Day | Dollar Amount | Required The member's maximum authorized cost divided by number of days in the care plan period automatically populates. |
| CDASS Effective Date Monthly Allocation Amt. |
Date (MM/DD/YY) Dollar Amount |
Required for MI, EBD 65+ and EBD-PD Enter CDASS information (All CDASS information must be entered in PPL's web portal). |
| Immediately prior to CCT enrollment, this client lived in a long-term care facility | Check box YesNo |
Required Check the appropriate box. |
| Case Manager Name | Text | Required Enter the name of the Case Manager. |
| Agency | Text | Required Enter the name of the agency. |
| Phone # | 10 Numbers 123-456-7890 |
Required Enter the phone number of the Case Manager. |
| Text | Required Enter the email address of the Case Manager. |
|
| Date | 6 Numbers (MM/DD/YY) |
Required Enter the date completed. |
| Case Manager's Supervisor Name | Text | Required Enter the name of the Case Manager's Supervisor. |
| Agency | Text | Required Enter the name of the agency. |
| Phone # | 10 Numbers 123-456-7890 |
Required Enter the phone number of the Case Manager's Supervisor. |
| Text | Required Enter the email address of the Case Manager's Supervisor. |
|
| Date | 6 Numbers (MM/DD/YY) |
Required Enter the date of PAR completion. |
Claim Submission
Refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down menu for general billing information, including claim submission information.
Paper Claim Reference Table
The following paper form reference table gives required and/or conditional fields for the paper CMS 1500 claim form for HCBS-CHCBS and CLLI claims:
| CMS Field Number & Label | Field is? | Instructions | ||||||||||||||||||||||||||||||||||
| 1. Insurance Type | Required | Place an "X" in the box marked as Medicaid. | ||||||||||||||||||||||||||||||||||
| 1a. Insured's ID Number | Required | Enter the member's Health First Colorado seven-digit Medicaid ID number as it appears on the Medicaid Identification card. Example: A123456. | ||||||||||||||||||||||||||||||||||
| 2. Patient's Name | Required | Enter the member's last name, first name, and middle initial. | ||||||||||||||||||||||||||||||||||
| 3. Patient's Date of Birth/Sex | Required | Enter the member's birth date using two digits for the month, two digits for the date, and two digits for the year. Example: 070114 for July 1, 2014. Place an "X" in the appropriate box to indicate the sex of the member. |
||||||||||||||||||||||||||||||||||
| 4. Insured's Name | Not required | |||||||||||||||||||||||||||||||||||
| 5. Patient's Address | Not Required | |||||||||||||||||||||||||||||||||||
| 6. Client Relationship to Insured | Not Required | |||||||||||||||||||||||||||||||||||
| 7. Insured's Address | Not Required | |||||||||||||||||||||||||||||||||||
| 8. Reserved for NUCC Use | Not Required | |||||||||||||||||||||||||||||||||||
| 9. Other Insured's Name | Not Required | |||||||||||||||||||||||||||||||||||
| 9a. Other Insured's Policy or Group Number | Not Required | |||||||||||||||||||||||||||||||||||
| 9b. Reserved for NUCC Use | ||||||||||||||||||||||||||||||||||||
| 9c. Reserved for NUCC Use | ||||||||||||||||||||||||||||||||||||
| 9d. Insurance Plan or Program Name | Not Required | |||||||||||||||||||||||||||||||||||
| 10a-c. Is patient's condition related to? | Not Required | |||||||||||||||||||||||||||||||||||
| 10d. Reserved for Local Use | ||||||||||||||||||||||||||||||||||||
| 11. Insured's Policy, Group or FECA Number | Not Required | |||||||||||||||||||||||||||||||||||
| 11a. Insured's Date of Birth, Sex | Not Required | |||||||||||||||||||||||||||||||||||
| 11b. Other Claim ID | Not Required | |||||||||||||||||||||||||||||||||||
| 11c. Insurance Plan Name or Program Name | Not Required | |||||||||||||||||||||||||||||||||||
| 11d. Is there another Health Benefit Plan? | Not Required | |||||||||||||||||||||||||||||||||||
| 12. Patient's or Authorized Person's signature | Required | Enter "Signature on File", "SOF", or legal signature. If there is no signature on file, leave blank or enter "No Signature on File". Enter the date the claim form was signed. |
||||||||||||||||||||||||||||||||||
| 13. Insured's or Authorized Person's Signature | Not Required | |||||||||||||||||||||||||||||||||||
| 14. Date of Current Illness Injury or Pregnancy | Not Required | |||||||||||||||||||||||||||||||||||
| 15. Other Date | Not Required | |||||||||||||||||||||||||||||||||||
| 16. Date Patient Unable to Work in Current Occupation | Not Required | |||||||||||||||||||||||||||||||||||
| 17. Name of Referring Physician | Conditional | |||||||||||||||||||||||||||||||||||
| 18. Hospitalization Dates Related to Current Service | Not Required | |||||||||||||||||||||||||||||||||||
| 19. Additional Claim Information | Conditional | |||||||||||||||||||||||||||||||||||
| 20. Outside Lab? $ Charges |
Not Required | |||||||||||||||||||||||||||||||||||
| 21. Diagnosis or Nature of Illness or Injury | Required | Enter at least one but no more than twelve diagnosis codes based on the member's diagnosis/condition. Enter applicable ICD-10 indicator. HCBS CHCBS and CLLI may use R69 |
||||||||||||||||||||||||||||||||||
| 22. Medicaid Resubmission Code | Conditional | List the original reference number for resubmitted claims. When resubmitting a claim, enter the appropriate bill frequency code in the left- hand side of the field. 7 - Replacement of prior claim 8 - Void/Cancel of prior claim This field is not intended for use for original claim submissions. |
||||||||||||||||||||||||||||||||||
| 23. Prior Authorization | Not Required | HCBS Leave blank |
||||||||||||||||||||||||||||||||||
| 24. Claim Line Detail | Information | The paper claim form allows entry of up to six detailed billing lines. Fields 24A through 24J apply to each billed line. Do not enter more than six lines of information on the paper claim. If more than six lines of information are entered, the additional lines will not be entered for processing. Each claim form must be fully completed (totaled). Do not file continuation claims (e.g., Page 1 of 2). |
||||||||||||||||||||||||||||||||||
| 24A. Dates of Service | Required | The field accommodates the entry of two dates: a "From" date of services and a "To" date of service. Enter the date of service using two digits for the month, two digits for the date and two digits for the year. Example: 010116 for January 1, 2016.
Single Date of Service: Enter the six digit date of service in the "From" field. Completion of the "To field is not required. Do not spread the date entry across the two fields. Span billing: permissible if the same service (same procedure code) is provided on consecutive dates. Waiver Services Providers should refer to specific billing instructions on the use of span billing. |
||||||||||||||||||||||||||||||||||
| 24B. Place of Service | Required | Enter the Place of Service (POS) code that describes the location where services were rendered. Health First Colorado accepts the CMS place of service codes.
|
||||||||||||||||||||||||||||||||||
| 24C. EMG | Not Required | |||||||||||||||||||||||||||||||||||
| 24D. Procedures, Services, or Supplies | Required | Enter the HCPCS procedure code that specifically describes the service for which payment is requested. Waiver Services Providers should refer to the member's approved Prior Authorization (PAR). |
||||||||||||||||||||||||||||||||||
| 24D. Modifier | Required | Enter the appropriate procedure-related modifier that applies to the billed service. Up to four modifiers may be entered when using the paper claim form. Waiver Services Providers should refer to the member's approved Prior Authorization (PAR). |
||||||||||||||||||||||||||||||||||
| 24E. Diagnosis Pointer | Required | Enter the diagnosis code reference letter (A-L) that relates the date of service and the procedures performed to the primary diagnosis. At least one diagnosis code reference letter must be entered. When multiple services are performed, the primary reference letter for each service should be listed first, other applicable services should follow. This field allows for the entry of 4 characters in the unshaded area. |
||||||||||||||||||||||||||||||||||
| 24F. $ Charges | Required | Enter the usual and customary charge for the service represented by the procedure code on the detail line. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. Some CPT procedure codes are grouped with other related CPT procedure codes. When more than one procedure from the same group is billed, special multiple pricing rules apply. The base procedure is the procedure with the highest allowable amount. The base code is used to determine the allowable amounts for additional CPT surgical procedures when more than one procedure from the same grouping is performed. Submitted charges cannot be more than charges made to non-Health First Colorado covered individuals for the same service. Do not deduct Health First Colorado co- payment or commercial insurance payments from the usual and customary charges. |
||||||||||||||||||||||||||||||||||
| 24G. Days or Units | Required | Enter the number of services provided for each procedure code. Enter whole numbers only- do not enter fractions or decimals. |
||||||||||||||||||||||||||||||||||
| 24G. Days or Units | General Instructions | A unit represents the number of times the described procedure or service was rendered. Except as instructed in this manual or in Health First Colorado bulletins, the billed unit must correspond to procedure code descriptions. The following examples show the relationship between the procedure description and the entry of units. Home & Community Based Services Combine units of services for a single procedure code for the billed time period on one detail line. Dates of service do not have to be reported separately. Example: If forty units of personal care services were provided on various days throughout the month of January, bill the personal care procedure code with a From Date of 01/03/XX and a To Date of 01/31/XX and 40 units. |
||||||||||||||||||||||||||||||||||
| 24H. EPSDT/Family Plan | Not Required | EPSDT shaded area) Not Required Family Planning (unshaded area) Not Required |
||||||||||||||||||||||||||||||||||
| 24I. ID Qualifier | Not Required | |||||||||||||||||||||||||||||||||||
| 24J. Rendering Provider ID # | Required | In the shaded portion of the field, enter the NPI of the Health First Colorado provider number assigned to the individual who actually performed or rendered the billed service. This number cannot be assigned to a group or clinic. | ||||||||||||||||||||||||||||||||||
| 25. Federal Tax ID Number | Not Required | |||||||||||||||||||||||||||||||||||
| 26. Patient's Account Number | Optional | Enter information that identifies the member or claim in the provider's billing system. Submitted information appears on the Remittance Advice (RA). | ||||||||||||||||||||||||||||||||||
| 27. Accept Assignment? | Required | The accept assignment indicates that the provider agrees to accept assignment under the terms of the payer's program. | ||||||||||||||||||||||||||||||||||
| 28. Total Charge | Required | Enter the sum of all charges listed in field 24F. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. | ||||||||||||||||||||||||||||||||||
| 29. Amount Paid | Not Required | |||||||||||||||||||||||||||||||||||
| 30. Rsvd for NUCC Use | ||||||||||||||||||||||||||||||||||||
| 31. Signature of Physician or Supplier Including Degrees or Credentials | Required | Each claim must bear the signature of the enrolled provider or the signature of a registered authorized agent. Each claim must have the date the enrolled provider or registered authorized agent signed the claim form. Enter the date the claim was signed using two digits for the month, two digits for the date and two digits for the year. Example: 070116 for July 1, 2016. |
||||||||||||||||||||||||||||||||||
| 32. 32- Service Facility Location Information 32a- NPI Number 32b- Other ID # |
Conditional | Enter the name, address and ZIP code of the individual or business where the member was seen or service was performed in the following format: 1st Line Name 2nd Line Address 3rd Line City, State and ZIP Code If the Provider Type is not able to obtain an NPI, enter the eight-digit Health First Colorado provider number of the individual or organization. |
||||||||||||||||||||||||||||||||||
| 33. Billing Provider Info & Ph # |
Required | Enter the name of the individual or organization that will receive payment for the billed services in the following format: 1st Line Name 2nd Line Address 3rd Line City, State and ZIP Code |
||||||||||||||||||||||||||||||||||
| 33a- NPI Number | Required | |||||||||||||||||||||||||||||||||||
| 33b- Other ID # | If the Provider Type is not able to obtain an NPI, enter the eight-digit Health First Colorado provider number of the individual or organization. | |||||||||||||||||||||||||||||||||||
CCT Procedure Code Table
Providers may bill the following procedure codes for the CCT program. Below is a breakdown of services by population.
| CCT- BI Services Procedure Code Table (Special Program Code 95) | |||
| Description | Procedure Code + Modifiers | Units | |
| Qualified Services | |||
| Adult Day Services | S5102 | UC | 1 unit = 1 day |
| Assistive Technology, per purchase | T2029 | UC, HB | 1 unit = 1 purchase |
| Behavioral Programming | H0025 | UC, TF | 1 unit = 30 minutes |
| CDASS (Cent/Unit) | T2025 | UC | 1 unit = 1 cent |
| CDASS Per Member/Per Month | T2040 | UC | 1 unit = 1 month |
| Day Treatment | H2018 | UC | 1 unit = 1 day |
| Home Modifications | S5165 | UC | 1 unit = 1 modification |
| Independent Living Skills Training (ILST) | T2013 | UC | 1 unit = 1 hour |
| Mental Health Counseling, Family | H0004 | UC, HR | 1 unit = 15 minutes |
| Mental Health Counseling, Group | H0004 | UC, HQ | 1 unit = 15 minutes |
| Mental Health Counseling, Individual | H0004 | UC | 1 unit = 15 minutes |
| Non-Medical Transportation, Taxi | A0100 | UC | 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Personal Care | T1019 | UC, TG | 1 unit = 15 minutes |
| Personal Emergency Response System (PERs), Install/Purchase | S5160 | UC | 1 unit = 1 purchase |
| PERs, Monitoring | S5161 | UC | 1 unit = 1 month of service |
| Relative Personal Care | T1019 | UC, HR, TG | 1 unit = 15 minutes |
| Respite Care, In Home | S5150 | UC | 1 unit = 15 minutes |
| Respite Care, NF | H0045 | UC, TF | 1 unit = 1 day |
| Substance Abuse Counseling, Family | T1006 | UC, HR, HF | 1 unit = 1 hour |
| Substance Abuse Counseling, Group | H0047 | UC, HQ, TF, HF | 1 unit = 1 hour |
| Substance Abuse Counseling, Individual | H0047 | UC, TF, HF | 1 unit = 1 hour |
| Supported Living Program | T2033 | UC | 1 unit = 1 day |
| Transitional Living, per day | T2016 | UC, HB | 1 unit = 1 day |
| Demonstration Services | |||
| Caregiver Education | S5110 | UC | 1 unit = 15 minutes |
| Community Transition Services, Coordinator | T2038 | UC | 1 unit = 1 transition |
| Community Transition Services, Items Purchased | A9900 | UC | 1 unit = 1 purchase |
| Home Delivered Meals | S5170 | UC | 1 unit = 1 delivery/meal |
| Intensive Case Management | T1016 | UC | 1 unit = 15 minutes |
| Peer Mentorship | H2015 | UC | 1 unit = 15 minutes |
| CCT- EBD 65+ Services Procedure Code Table (Special Program Code 95) | |||
| Description | Procedure Code + Modifiers | Units | |
| Qualified Services | |||
| Adult Day Services, Basic | S5105 | UC | 1 unit = 4-5 hours |
| Adult Day Services, Specialized | S5105 | UC, TF | 1 unit = 3-5 hours |
| Consumer Directed Attendant Support Services (CDASS), (Cent/Unit) | T2025 | UC | 1 unit = 1 cent |
| CDASS Per Member/ Per Month (PM/PM) | T2040 | UC | 1 unit = 1 month |
| Home Modifications | S5165 | UC | 1 unit = 1 modification |
| Homemaker | S5130 | UC | 1 unit = 15 minutes |
| IHSS Health Maintenance Activities | H0038 | UC | 1 unit = 15 minutes |
| IHSS Homemaker | S5130 | UC, KX | 1 unit = 15 minutes |
| IHSS Personal Care | T1019 | UC, KX | 1 unit = 15 minutes |
| IHSS Relative Personal Care | T1019 | UC, HR, KX | 1 unit = 15 minutes |
| Medication Reminder, Install/Purchase | T2029 | UC, TF | 1 unit = 1 purchase |
| Medication Reminder, Monitoring | S5185 | UC | 1 unit = 1 month |
| Non-Medical Transportation, Taxi | A0100 | UC | 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Personal Care | T1019 | UC | 1 unit = 15 minutes |
| Personal Emergency Response System (PERs), Install/Purchase | S5160 | UC | 1 unit =1 purchase |
| PERs, Monitoring | S5161 | UC | 1 unit = 1 month |
| Relative Personal Care | T1019 | UC, HR | 1 unit = 15 minutes |
| Respite Care, ACF | S5151 | UC | 1 unit = 1 day |
| Respite Care, In Home | S5150 | UC | 1 unit = 15 minutes |
| Respite Care, NF | H0045 | UC | 1 unit = 1 day |
| Demonstration Services | |||
| Caregiver Education | S5110 | UC | 1 unit = 15 minutes |
| Community Transition Services, Coordinator | T2038 | UC | 1 unit = 1 transition |
| Community Transition Services, Items Purchased | A9900 | UC | 1 unit = 1 purchase |
| Home Delivered Meals | S5170 | UC | 1 unit = 1 delivery/meal |
| Independent Living Skills Training (ILST) | H2014 | UC | 1 unit = 15 minutes |
| Intensive Case Management | T1016 | UC | 1 unit = 15 minutes |
| Peer Mentorship | H2015 | UC | 1 unit = 15 minutes |
| Transitional Behavioral Health Supports | H0025 | UC | 1 unit = 30 minutes |
| CCT- EBD 18- 64 Services Procedure Code Table (Special Program Code 95) | |||
| Description | Procedure Code + Modifiers | Units | |
| Qualified Services | |||
| Adult Day Services, Basic | S5105 | UC | 1 unit = 4-5 hours |
| Adult Day Services, Specialized | S5105 | UC, TF | 1 unit = 3-5 hours |
| Consumer Directed Attendant Support Services (CDASS), (Cent/Unit) | T2025 | UC | 1 unit = 1 cent |
| CDASS Per Member/ Per Month (PM/PM) | T2040 | UC | 1 unit = 1 month |
| Home Modifications | S5165 | UC | 1 unit = 1 modification |
| Homemaker | S5130 | UC | 1 unit = 15 minutes |
| IHSS Health Maintenance Activities | H0038 | UC | 1 unit = 15 minutes |
| IHSS Homemaker | S5130 | UC, KX | 1 unit = 15 minutes |
| IHSS Personal Care | T1019 | UC, KX | 1 unit = 15 minutes |
| IHSS Relative Personal Care | T1019 | UC, HR, KX | 1 unit = 15 minutes |
| Medication Reminder, Install/Purchase | T2029 | UC, TF | 1 unit = 1 purchase |
| Medication Reminder, Monitoring | S5185 | UC | 1 unit = 1 month |
| Non-Medical Transportation, Taxi | A0100 | UC | 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Personal Care | T1019 | UC | 1 unit = 15 minutes |
| Personal Emergency Response System (PERs), Install/Purchase | S5160 | UC | 1 unit =1 purchase |
| PERs, Monitoring | S5161 | UC | 1 unit = 1 month |
| Relative Personal Care | T1019 | UC, HR | 1 unit = 15 minutes |
| Respite Care, ACF | S5151 | UC | 1 unit = 1 day |
| Respite Care, In Home | S5150 | UC | 1 unit = 15 minutes |
| Respite Care, NF | H0045 | UC | 1 unit = 1 day |
| Demonstration Services | |||
| Caregiver Education | S5110 | UC | 1 unit = 15 minutes |
| Community Transition Services, Coordinator | T2038 | UC | 1 unit = 1 transition |
| Community Transition Services, Items Purchased | A9900 | UC | 1 unit = 1 purchase |
| Home Delivered Meals | S5170 | UC | 1 unit = 1 delivery/meal |
| Independent Living Skills Training (ILST) | H2014 | UC | 1 unit = 15 minutes |
| Intensive Case Management | T1016 | UC | 1 unit = 15 minutes |
| Peer Mentorship | H2015 | UC | 1 unit = 15 minutes |
| Transitional Behavioral Health Supports | H0025 | UC | 1 unit = 30 minutes |
| CCT- CMHS Services Procedure Code Table (Special Program Code 95) | |||
| Description | Procedure Code + Modifiers | Units | |
| Qualified Services | |||
| Adult Day Services, Basic | S5105 | UC | 1 unit = 4-5 hours |
| Adult Day Services, Specialized | S5105 | UC, TF | 1 unit = 3-5 hours |
| Consumer Directed Attendant Support Services (CDASS), (Cent/Unit) | T2025 | UC | 1 unit = 1 cent |
| CDASS Per Member/ Per Month (PM/PM) | T2040 | UC | 1 unit = 1 month |
| Home Modifications | S5165 | UC | 1 unit = 1 modification |
| Homemaker | S5130 | UC | 1 unit = 15 minutes |
| Medication Reminder, Install/Purchase | T2029 | UC, TF | 1 unit = 1 purchase |
| Medication Reminder, Monitoring | S5185 | UC | 1 unit = 1 month |
| Non-Medical Transportation, Taxi | A0100 | UC | 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Mobility Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0120 A0120 A0120 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT UC, TN |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Non-Medical Transportation, Wheelchair Van To and From Adult Day | |||
| Mileage Band 1 (0-10 miles) Mileage Band 2 (11-20 miles) Mileage Band 3 (over 20 miles) |
A0130 A0130 A0130 |
UC UC, TT, HB UC, TN, HB |
1 unit = 1-way trip 1 unit = 1-way trip 1 unit = 1-way trip |
| Personal Care | T1019 | UC | 1 unit = 15 minutes |
| Personal Emergency Response System (PERs), Install/Purchase | S5160 | UC | 1 unit =1 purchase |
| PERs, Monitoring | S5161 | UC | 1 unit = 1 month |
| Relative Personal Care | T1019 | UC, HR | 1 unit = 15 minutes |
| Respite Care, ACF | S5151 | UC | 1 unit = 1 day |
| Respite Care, NF | H0045 | UC | 1 unit = 1 day |
| Demonstration Services | |||
| Caregiver Education | S5110 | UC | 1 unit = 15 minutes |
| Community Transition Services, Coordinator | T2038 | UC | 1 unit = 1 transition |
| Community Transition Services, Items Purchased | A9900 | UC | 1 unit = 1 purchase |
| Home Delivered Meals | S5170 | UC | 1 unit = 1 delivery/meal |
| Independent Living Skills Training (ILST) | H2014 | UC | 1 unit = 15 minutes |
| Intensive Case Management | T1016 | UC | 1 unit = 15 minutes |
| Peer Mentorship | H2015 | UC | 1 unit = 15 minutes |
| Transitional Behavioral Health Supports | H0025 | UC | 1 unit = 30 minutes |
| CCT- DD Services Procedure Code Table (Special Program Code 95) | ||||
| Description | Procedure Code | Modifiers | Level | Units |
| Qualified Services | ||||
| Behavioral Services | ||||
| Line Service | H2019 | UC | 1 unit = 15 minutes | |
| Behavioral Consultation | H2019 | UC, HI, TG | 1 unit = 15 minutes | |
| Behavioral Counseling, Individual | H2019 | UC, TF, TG | 1 unit = 15 minutes | |
| Behavioral Counseling, Group | H2019 | UC, TF, HQ | 1 unit = 15 minutes | |
| Behavioral Plan Assessment | T2024 | UC, HI | 1 unit = 15 minutes | |
| Day Habilitation | ||||
| Specialized Day Habilitation | T2021 T2021 T2021 T2021 T2021 T2021 T2021 |
UC, HQ UC,HI, HQ UC, TF, HQ UC, TF, HI, HQ UC, TG, HQ UC, TG, HI, HQ UC, SC, HQ |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 Level 7 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Supported Community Connections | T2021 T2021 T2021 T2021 T2021 T2021 T2021 |
UC UC, HI UC, TF UC, TF, HI UC, TG UC, TG, HI UC, SC |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 Level 7 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Dental | ||||
| Dental, Basic/ Preventive | D2999 | UC, HI | 1 unit = 1 dollar | |
| Dental, Major | D2999 | UC, TF | 1 unit = 1 dollar | |
| Non-Medical Transportation | ||||
| To/From Day Program, Mileage Range | T2003 T2003 T2003 |
UC UC, HI UC, TF |
0-10 Miles 11-20 Miles 21- up Miles |
1 unit = 2 trips per day 1 unit = 2 trips per day 1 unit = 2 trips per day |
| Other (Public Conveyance) | T2004 | UC | 1 unit = 1 dollar | |
| Pre-Vocational Services | ||||
| Pre-Vocational Services | T2015 T2015 T2015 T2015 T2015 T2015 |
UC, HQ UC, HI, HQ UC, TF, HQ UC, TF, HI, HQ UC, TG, HQ UC, TG, HI, HQ |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Residential Services | ||||
| Group Home | T2016 T2016 T2016 T2016 T2016 T2016 T2016 |
UC, HQ UC, HI, HQ UC, TF, HQ UC, TF, HI, HQ UC, TG, HQ UC, TG, HI, HQ UC, SC, HQ |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 Level 7 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Personal Care Alternative | T2016 T2016 T2016 T2016 T2016 T2016 T2016 |
UC UC, HI UC, TF UC, TF, HI UC, TG UC, TG, HI UC, SC |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 Level 7 |
1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = 1 day |
| Host Home | T2016 T2016 T2016 T2016 T2016 T2016 T2016 |
UC, TT UC, HI, TT UC, TF, TT UC, TF, HI, TT UC, TG, TT UC, TG, HI, TT UC, SC, TT |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 Level 7 |
1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = 1 day 1 unit = individual approved rate |
| Supported Employment | ||||
| Supported Employment, Individual, All Levels (1-6) | T2019 | UC, SC | All Levels (1-6) | 1 unit = 15 minutes |
| Supported Employment, Group | T2019 T2019 T2019 T2019 T2019 T2019 |
UC, HQ UC, HI, HQ UC, TF, HQ UC, TF, HI, HQ UC, TG, HQ UC, TG, HI, HQ |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Job Development, Individual, Level 1-2 | H2023 | UC | Level 1-2 | 1 unit = 15 minutes |
| Job Development, Individual, Level 3-4 | H2023 | UC, HI | Level 3-4 | 1 unit = 15 minutes |
| Job Development, Individual, Level 5-6 | H2023 | UC, TF | Level 5-6 | 1 unit = 15 minutes |
| Job Development, Group, All Levels | H2023 | UC, HQ | All Levels (1-6) | 1 unit = 15 minutes |
| Job Placement, Individual, All Levels (1-6) | H2024 | UC | All Levels (1-6) | 1 unit = 1 dollar |
| Job Placement, Group, All Levels (1-6) | H2024 | UC, HQ | All Levels (1-6) | 1 unit = 1 dollar |
| Specialized Medical Equipment | ||||
| Specialized Medical Equipment and Supplies, Disposable | T2028 | UC | 1 unit = 1 dollar | |
| Specialized Medical Equipment | T2029 | UC, TF | 1 unit = 1 dollar | |
| Vision | V2799 | UC, HI | 1 unit = 1 dollar | |
| Demonstration Services | ||||
| Assistive Technology, Extended | T2029 | UC | 1 unit = 1 purchase | |
| Caregiver Education | S5110 | UC | 1 unit = 15 minutes | |
| Community Transition Services, Coordinator | T2038 | UC | 1 unit = 1 transition | |
| Community Transition Services, Items Purchased | A9900 | UC | 1 unit = 1 purchase | |
| Intensive Case Management | T1016 | UC | 1 unit = 15 minutes | |
| Peer Mentorship | H2015 | UC | 1 unit = 15 minutes | |
| CCT- SLS Services Procedure Code Table (Special Program Code 95) | ||||
| Description | Procedure Code | Modifiers | Level | Units |
| Qualified Services | ||||
| Assistive Technology * | T2035 | UC | 1 unit = 1 dollar | |
| Mentorship | H2021 | UC | 1 unit = 15 minutes | |
| Personal Care | T1019 | UC, TF | 1 unit = 15 minutes | |
| Personal Emergency Response (PERs) | S5161 | UC | 1 unit = 1 dollar | |
| Vehicle Modifications * | T2039 | UC | 1 unit = 1 dollar | |
| Vision * | V2799 | UC, HI | 1 unit = 1 dollar | |
| Behavioral Services | ||||
| Line Services | H2019 | UC | 1 unit = 15 minutes | |
| Behavioral Consultation | H2019 | UC, HI, TG | 1 unit = 15 minutes | |
| Behavioral Counseling, Group | H2019 | UC, TF, HQ | 1 unit = 15 minutes | |
| Behavioral Counseling, Individual | H2019 | UC, TF, TG | 1 unit = 15 minutes | |
| Behavioral Plan Assessment | T2024 | UC, HI | 1 unit = 15 minutes | |
| Day Habilitation | ||||
| Specialized Day Habilitation | T2021 T2021 T2021 T2021 T2021 T2021 |
UC, HQ UC. HI, HQ UC, TF, HQ UC, TF, HI, HQ UC, TG, HQ UC, TG, HI, HQ |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Supported Community Connections | T2021 T2021 T2021 T2021 T2021 T2021 |
UC UC, HI UC, TF UC, TF, HI UC, TG UC, TG, HI |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Dental | ||||
| Dental, Basic/ Preventive Services * | D2999 | UC, HI | 1 unit = 1 dollar | |
| Dental, Major Services * | D2999 | UC, TF | 1 unit = 1 dollar | |
| Homemaker | ||||
| Homemaker, Basic | S5130 | UC, HI | 1 unit = 15 minutes | |
| Homemaker, Enhanced | S5130 | UC, TF | 1 unit = 15 minutes | |
| Home Accessibility Adaptations * | S5165 | UC | 1 unit = 1 dollar | |
| Non-Medical Transportation | ||||
| To/From Day Program, Mileage Range * | T2003 T2003 T2003 |
UC UC, HI UC, TF |
0-10 Miles 11-20 Miles 21- up Miles |
1 unit = 2 trips per day 1 unit = 2 trips per day 1 unit = 2 trips per day |
| Mileage Not Day Program * | T2003 | UC, HB | 1 unit = 4 trips per week | |
| Other (Public Conveyance) * | T2004 | UC | 1 unit = 1 dollar | |
| Pre-Vocational Services | ||||
| Pre-Vocational Services | T2015 T2015 T2015 T2015 T2015 T2015 |
UC, HQ UC, HI, HQ UC, TF, HQ UC, TF, HI, HQ UC, TG, HQ UC, TG, HI, HQ |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Professional Services | ||||
| Massage Therapy | 97124 | UC | 1 unit = 15 minutes | |
| Movement Therapy, Bachelor's Degree | G0176 | UC, HN | 1 unit = 15 minutes | |
| Movement Therapy, Master's Degree | G0176 | UC | 1 unit = 15 minutes | |
| Hippotherapy, Group | S8940 | UC, HQ | 1 unit = 15 minutes | |
| Hippotherapy, Individual | S8940 | UC | 1 unit = 15 minutes | |
| Rec Pass, Access Fee | S5199 | UC | 1 unit = 1 dollar | |
| Respite Services | ||||
| Respite Care, Camp | T2036 | UC | 1 unit = 1 dollar | |
| Respite Care, Group | S5151 | UC, HQ, TG | 1 unit = 1 dollar | |
| Respite Care, Individual, 15 Minutes | S5150 | UC, TG | 1 unit = 15 minutes | |
| Respite Care, Individual, Day | S5151 | UC, TG | 1 unit = 1 dollar | |
| Specialized Medical Equipment and Supplies | ||||
| Specialized Medical Equipment and Supplies, Disposable | T2028 | UC | 1 unit = 1 dollar | |
| Specialized Medical Equipment | T2029 | UC, TF | 1 unit = 1 dollar | |
| Supported Employment | ||||
| Supported Employment, Individual, All Levels (1-6) | T2019 | UC, HI | All Levels (1-6) | 1 unit = 15 minutes |
| Supported Employment, Group | T2019 T2019 T2019 T2019 T2019 T2019 |
UC, HQ UC, HI, HQ UC, TF, HQ UC, TF, HI, HQ UC, TG, HQ UC, TG, HI, HQ |
Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 |
1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes 1 unit = 15 minutes |
| Job Development, Individual, Level 1-2 | H2023 | UC | Level 1-2 | 1 unit = 15 minutes |
| Job Development, Individual, Level 3-4 | H2023 | UC, HI | Level 3-4 | 1 unit = 15 minutes |
| Job Development, Individual, Level 5-6 | H2023 | UC, TF | Level 5-6 | 1 unit = 15 minutes |
| Job Development, Group, All Levels | H2023 | UC, HQ | All Levels (1-6) | 1 unit = 15 minutes |
| Job Placement, Individual, All Levels (1-6) | H2024 | UC | All Levels (1-6) | 1 unit = 1 dollar |
| Job Placement, Group, All Levels (1-6) | H2024 | UC, HQ | All Levels (1-6) | 1 unit = 1 dollar |
| Demonstration Services | ||||
| Caregiver Education | S5110 | UC | 1 unit = 15 minutes | |
| Community Transition Services, Coordinator * | T2038 | UC | 1 unit = 1 transition | |
| Community Transition Services, Items Purchased * | A9900 | UC | 1 unit = 1 purchase | |
| Independent Living Skills Training (ILST) | H2014 | UC | 1 unit = 15 minutes | |
| Intensive Case Management * | T1016 | UC | 1 unit = 15 minutes | |
| * Outside of Service Plan Authorization Limit (SPAL) | ||||
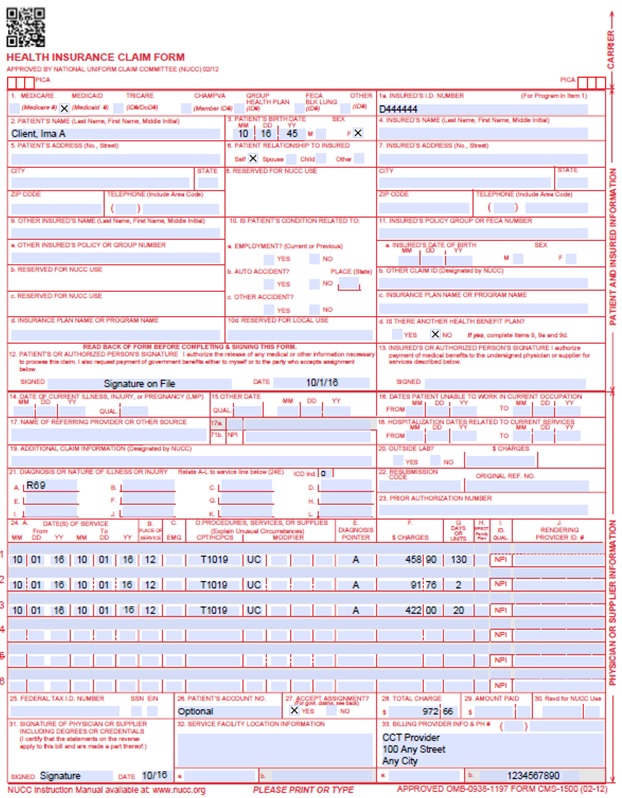
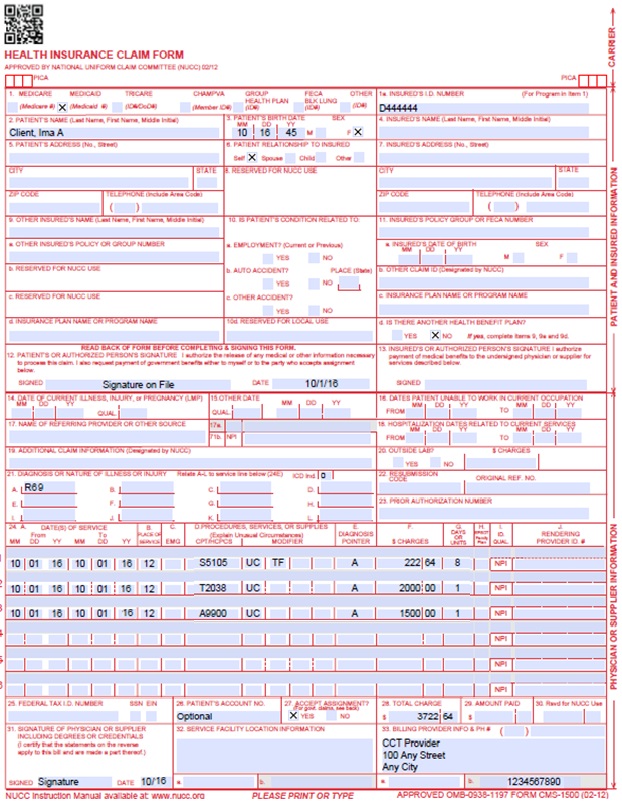
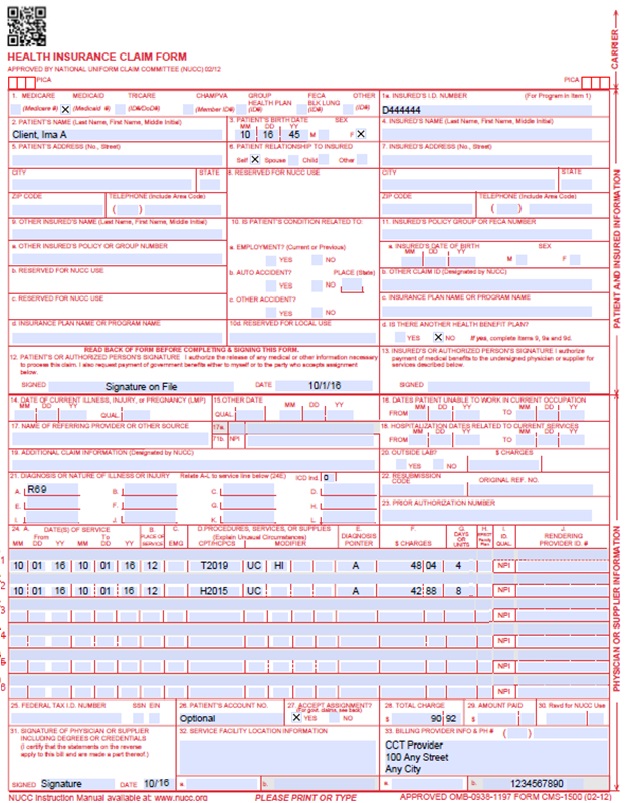
CCT Claim Examples
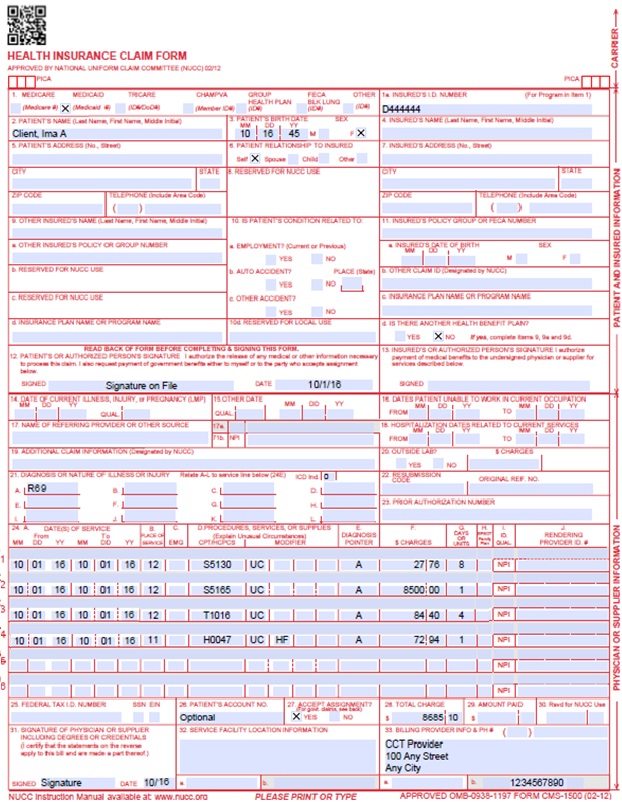
CMS 1500 CCT-BI Claim Example
CMS 1500 CCT-CMHS Claim Example
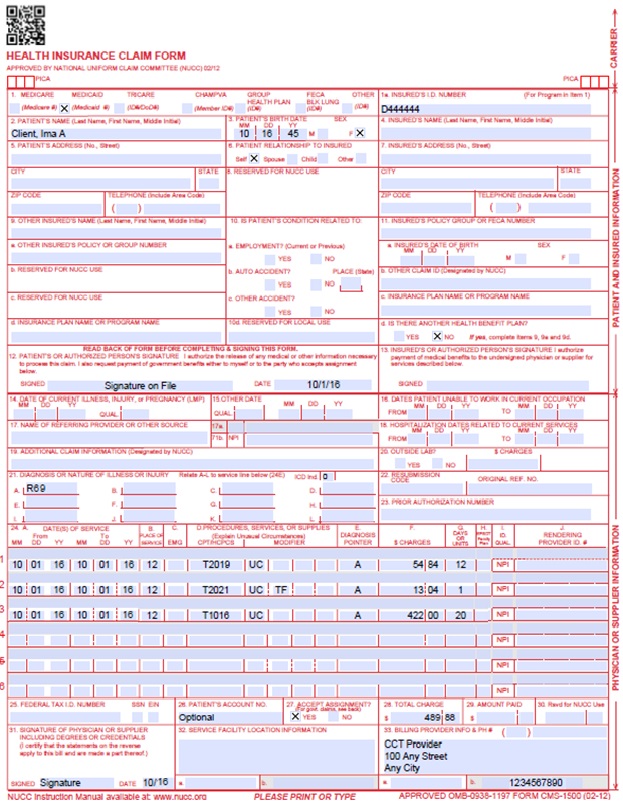
CMS 1500 CCT-DD Claim Example
CMS 1500 CCT-EBD (18-64) Claim Example
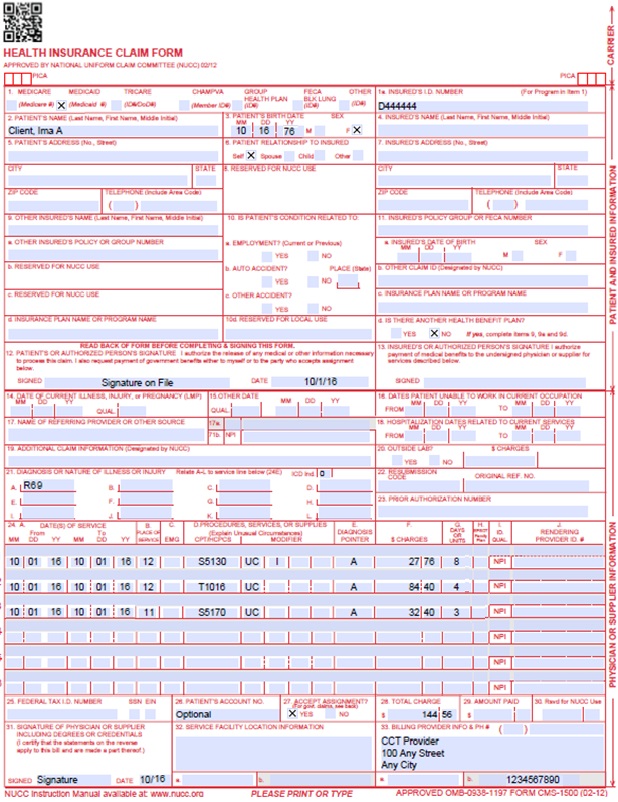
CMS 1500 CCT-EBD (65+) Claim Example
CMS 1500 CCT-SLS Claim Example
Timely Filing
For more information on timely filing policy, including the resubmission rules for denied claims, refer to the General Provider Information Manual located on the Billing Manuals web page under the General Provider Information drop-down menu.
Colorado Choice Transitions Program Revision Log
| Revision Date | Addition/Changes | Made by |
| 12/1/2016 | Manual revised for interChange implementation. For manual revisions prior to 12/01/2016, please refer to Archive. | HPE (now DXC) |
| 12/27/2016 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_2.xlsx | HPE (now DXC) |
| 1/10/2017 | Updates based on Colorado iC Stage Provider Billing Manual Comment Log v0_3.xlsx | HPE (now DXC) |
| 1/19/2017 | Updates based on Colorado iC Stage Provider Billing Manual Comment Log v0_4.xlsx | HPE (now DXC) |
| 1/26/2017 | Updates based on Department 1/20/2017 approval email | HPE (now DXC) |
| 5/22/2017 | Updates based on Fiscal Agent name change from HPE to DXC | DXC |
| 6/26/2018 | Updated Timely Filing Removal of information duplicated from general manual |
HCPF |
| 6/28/2018 | Minor grammatical updates | HCPF |
| 12/21/2018 | Clarification to signature requirements | HCPF |
| 3/19/2018 | Clarification to signature requirements | HCPF |
| 3/12/2020 | Converted to web page | HCPF |
| 9/14/2020 | Added Line to Box 32 under the Paper Claim Reference Table | HCPF |