Support Post-COVID Recovery & HCBS Innovation
The Need
The COVID-19 pandemic has had a startling, disproportionate impact on individuals residing in congregate care settings. While the American Rescue Plan Act (ARPA) funding may not be used for nursing facilities, it may be used to transform community-based residential care settings.
Reimagining Colorado’s residential settings is required to support member health, safety, and overall well-being, as well as to create the long-term care system of the future. This future system ideally supports choice, offers the continuum of care, and is provided in the member’s home or community of choice. The ARPA funding will support collaboration with community partners to begin the work of transforming the residential care setting environment and method by which these partners provide services.
Though higher rates and wages are important for sustainability, there are often specific projects that require a more significant upfront investment. With an eye toward promoting innovation, grants will be made available for one-time, transformative initiatives. Additionally, funding will be used to address specific barriers to the receipt of ongoing care in a member’s home or other community-based setting. An example would be the need for home modifications to adapt a person’s physical space or access to a personal care attendant to support a person to live independently. Initiatives that strengthen these services and supports will be worthwhile investments as they extend the time members can live and thrive in their home of choice.

Initiative 4.01. - Residential Innovation
Read a more in-depth summary of this project's outcomes

Initiative 4.02. - Promote Single Occupancy
Read a more in-depth summary of this project's outcomes
Initiative 4.03 - Child/Youth Step-down Options Program and Provider Recruitment
Read a more in-depth summary of this project's outcomes
Initiative 4.04 - Tiered Residential Rates and Benefits
Read a more in-depth summary of this project's outcomes
Initiative 4.05 - Pilot CAPABLE
Read a more in-depth summary of this project's outcomes
Initiative 4.06 - Supported Employment Pilot Extension
Read a more in-depth summary of this project's outcomes
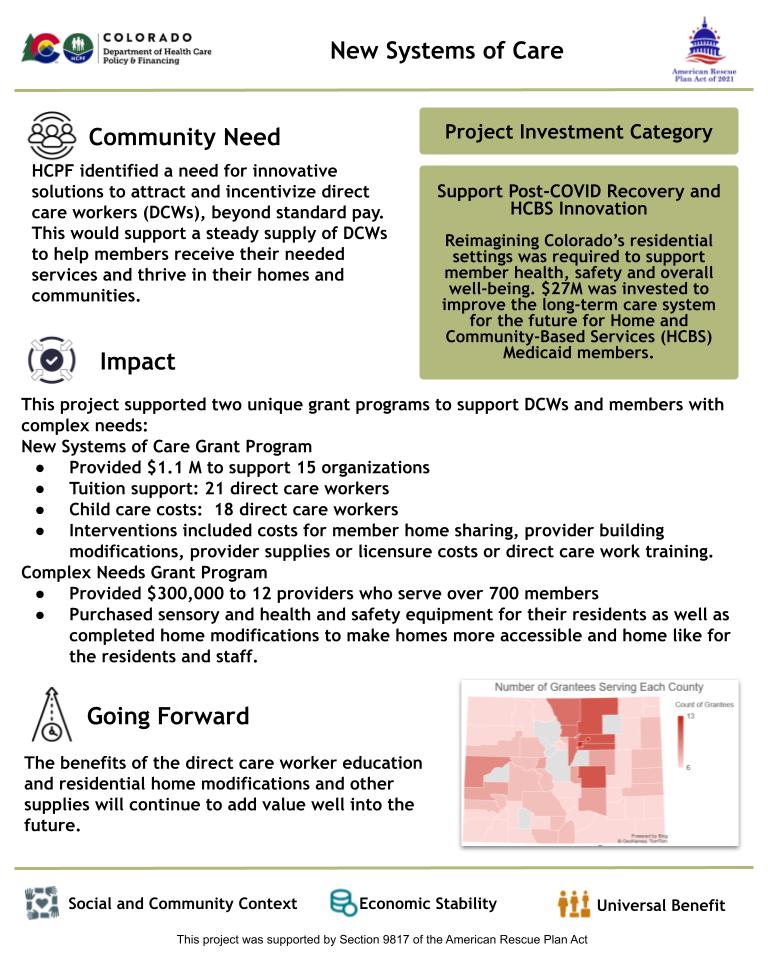
Initiative 4.07 - New Systems of Care
Read a more in-depth summary of this project's outcomes
Initiative 4.08 - Respite Grant Program
Read a more in-depth summary of this project's outcomes
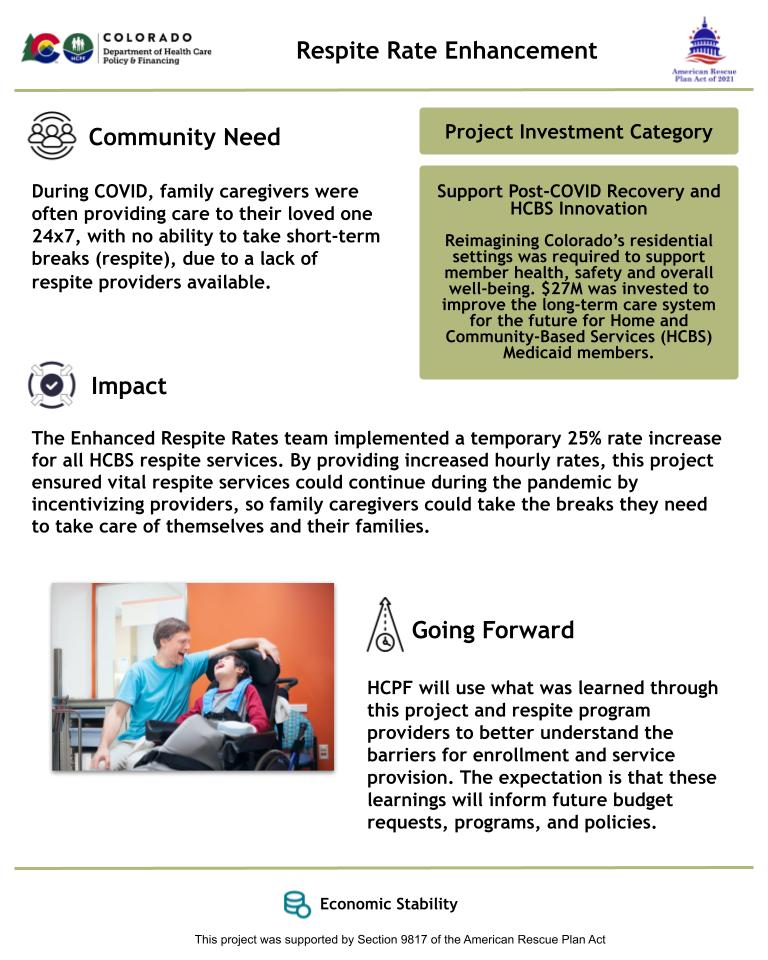
Initiative 4.09 - Respite Rate Enhancement
Read a more in-depth summary of this project's outcomes
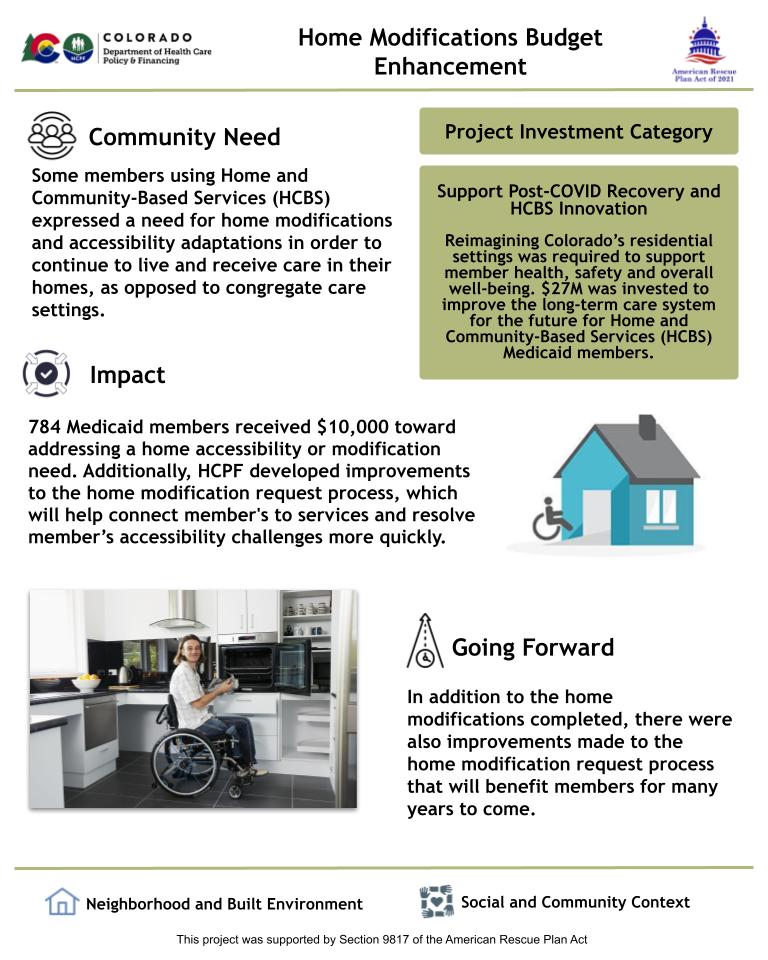
Initiative 4.10 - Home Modification Budget Enhancement
Read a more in-depth summary of this project's outcomes
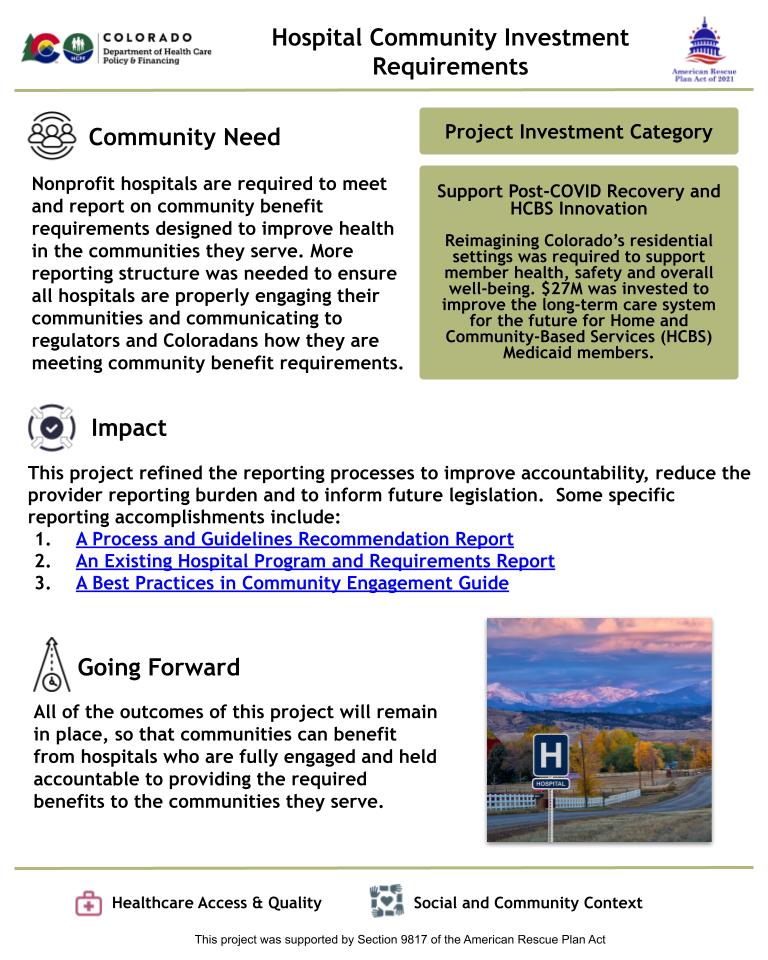
Initiative 4.11 - Hospital Community Investment Requirements
Read a more in-depth summary of this project's outcomes
Initiative 4.12 - Community First Choice
Read a more in-depth summary of this project's outcomes