- Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Program
- General Billing Information
- General Program Provisions
- Services
- ColoradoPAR Prior Authorization Requests (PARs)
- Benefits
- Billing Guidelines
- CMS 1500 Paper Claim Instructions
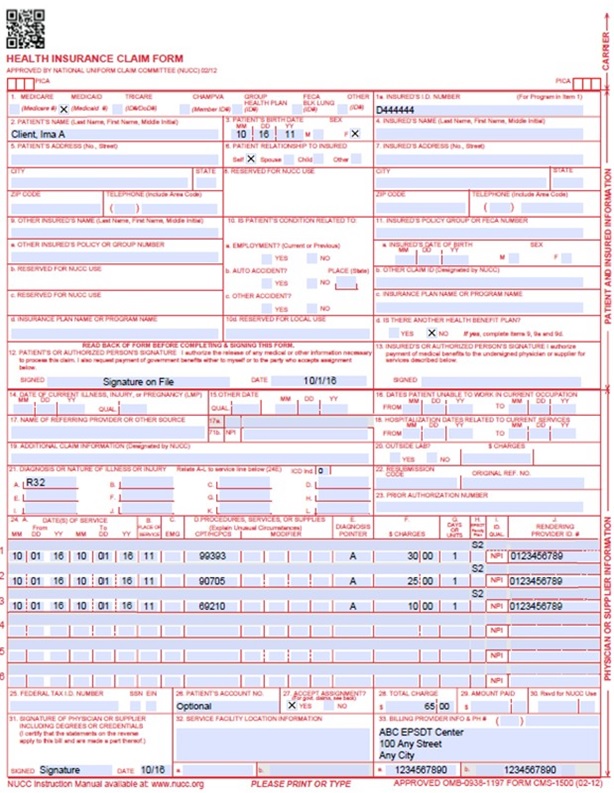
- CMS 1500 EPSDT Claim Example
- Timely Filing
- EPSDT Revisions Log
Return to Billing Manuals Web Page
Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Program
Providers must be enrolled as a Health First Colorado (Colorado's Medicaid Program) provider in order to:
- Treat a Health First Colorado member
- Submit claims for payment to Health First Colorado
The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit provides comprehensive and preventive health care services for children and youth ages 20 and under, who are enrolled in Health First Colorado. EPSDT is key to ensuring that children and youth receive appropriate preventive, dental, mental health, developmental and specialty services.
| Early | Assessing and identifying problems early |
| Periodic | Checking children's health at periodic, age-appropriate intervals |
| Screening | Providing physical, mental, developmental, dental, hearing, vision, and other screening tests to detect potential problems |
| Diagnostic | Performing diagnostic tests to follow up when a risk is identified |
| Treatment | Control, correct or reduce health problems found |
One of the goals of EPSDT is to establish a regular pattern of healthcare through routine health screenings, diagnostic, and treatment services.
All states are required to complete a report to the federal government on April 1 of each year as to the numbers of services received by the EPSDT eligible members. All states have a minimum requirement of 80% of the children and youth receiving at least one screening visit per year.
Providers should refer to the Code of Colorado Regulations, Program Rules (10 CCR 2505-10.8.280), for specific information when providing EPSDT care.
Accountability of services shall be maintained through medical records and documentation used in informing, screening, diagnosis and treatment services. The provider who is performing the screening must maintain medical records specific to EPSDT screening services that:
- Contain the results of all diagnostic tests and reports of all consultations.
- Contain the reason for visit, e.g., screening, follow-up, etc.
- Contain the date screening services were performed, and documentation of the specific tests or procedures performed, along with the results of these tests and procedures.
- Contain documentation of any screening service that was due but not completed and the medical contraindication or other reason why it was not completed.
- Contain documentation of declination of screening services by parents.
- Contain referrals made for diagnosis, treatment, or other medically necessary health services for conditions as a result of a screening service.
- Contain the date next screening is due.
- Contain the documentation of direct referral for age-appropriate dental services.
General Billing Information
Refer to the General Provider Information manual for general billing information.
General Program Provisions
A comprehensive EPSDT Periodic Screening examination includes the following components:
- Comprehensive health & developmental history
- Immunizations appropriate to age & health history
- Comprehensive unclothed physical examination
- Laboratory tests (including lead blood level assessment appropriate to age & risk)
- Assessment of physical, emotional & developmental growth
- Assessment of mental/behavioral health
- Assessment of mouth, oral cavity and teeth, including referral to a dentist
- Hearing assessment
- Assessment of nutritional status
- Family planning services and adolescent maternity care
- Vision assessment
- Health education (including anticipatory guidance)
- Treatment and referrals for any medically necessary further diagnosis and treatment
Types of EPSDT Provider Visits
- Periodic Screen
The periodic screen includes comprehensive health assessments that are performed soon after birth or as early as possible in a child's life. It is repeated at prescribed intervals until the age of 20, as described in the AAP Bright Futures Periodicity Schedule. - Inter-Periodic Visit
An inter-periodic visit is any other healthcare visit the child may need, such as visits for an earache, fever or injury. Additional visits, or "inter-periodic" screens, may become necessary if circumstances suggest the need for more screens, or to bring a child who has missed one or more periodic screens into compliance. Medically necessary inter-periodic screens must be provided to determine the existence of suspected physical, or mental illnesses or conditions. The determination of whether an inter-periodic screen is medically necessary may be made by a health, developmental or educational professional who comes into contact with the child outside of the formal health care system (e.g., special education programs, Head Start and daycare programs, the Special Supplemental Food Program for Women, Infants and Children (WIC) and other nutritional assistance programs).
Outreach and Case Management - Healthy Communities Program
Each family or member is assigned to a Family Health Coordinator in their local area. The Family Health Coordinator's services are a part of the member's Health First Colorado benefit and offers support services, including the following:
- Ensures that members are informed of program benefits.
- Assists child in accessing health care services within a reasonable time period.
- Offers assistance in identifying participating Health First Colorado doctors, dentists, other medical specialists and managed care programs or Accountable Care Programs. Assists in making and reminds members of appointments, if requested.
- Follows up on appointments that may have been missed, if requested by a provider.
- Assists with connecting child with non-medical community resources.
- Coordinate the following types of health care services wherever possible:
- Newborn or well-baby check-ups
- Daycare or Head Start physicals
- Routine well-child physical exams
- Dental Screenings
- Behavioral Health screenings
- Developmental screenings
Visit the Healthy Communities web page on the Department's website to find a Family Health Coordinator in your area.
As a provider under a Regional Accountable Entity (RAE), you also have the ability to access medical case management through those organizations. Please visit the Health First Colorado Regional Organization web page for more information.
Services
EPSDT is made up of the following screening, diagnostic, and treatment services:
Screening Services
Comprehensive Health and Developmental History
At the initial screen, the provider should obtain a comprehensive health, developmental, behavioral, mental health and nutritional history from the child's parents or guardians. The comprehensive initial history should include the following information:
- Family medical history
- Member medical history, including prenatal problems, neonatal problems, developmental milestones, surgeries, current medication and current health problems
- Immunization history
- Nutritional history
- Social history
- Living conditions
- Family and member history of behavioral problems
This information should be updated at every well child check.
Comprehensive unclothed physical exam
Unclothed Physical Inspection - Check the general appearance of the child to determine overall health status. This process can pick up obvious physical defects, including orthopedic disorders, hernia, skin disease, and genital abnormalities. Physical inspection includes an examination of all organ systems such as pulmonary, cardiac, and gastrointestinal. Please visit the AAP Bright Futures Periodicity Schedule for more information at the Bright Futures Clinical Practice web page.
Appropriate immunizations (according to the Advisory Committee on Immunization Practices)
The National Vaccines for Children Program (VFC) supplies most vaccines at no cost to physicians enrolled in the VFC program. All PCPs participating in Health First Colorado (including those in Managed Care Organizations) are eligible to enroll and participate in the VFC program.
Oral Health Screening Services
Dental screening services, such as oral health assessments, can be provided during a well-child visit by the pediatric primary care provider.
Laboratory tests (including REQUIRED lead toxicity testing)
Identify the minimum laboratory tests or analyses to be performed by medical providers for particular age or population groups. Physicians providing screening/assessment services under the EPSDT benefit use their medical judgment in determining the applicability of the laboratory tests or analyses to be performed.
Federal regulations require that all Health First Colorado-enrolled children have a blood lead test at 12 and 24 months of age. CMS requires the use of the blood lead test when screening children for lead poisoning.
If a child between the ages of 24 months and 72 months has not received a screening blood lead test, the child must receive it immediately.
If a child is found to have blood lead levels equal to or greater than 10 ug/dl, providers are to use their professional judgment, with reference to CDC guidelines covering member management and treatment, including follow up blood tests and initiating investigations to determine the source of lead, where indicated. Determining the source of lead may be completed by your local public health agency. For more information please visit the Colorado Department of Public Health and Environment's website.
Vision and Hearing Screening Services
Subjective vision and hearing screens should be performed at every well-child visit or based on an assessment of risk. If medically indicated, the subjective screens can lead to inter-periodic screens or a referral to a specialist if a problem is identified.
Developmental Surveillance and Screening Services
According to the American Academy of Pediatrics, developmental surveillance is a flexible, longitudinal, continuous, and cumulative process whereby knowledgeable health care professionals identify children who may have developmental problems. Developmental surveillance should include the following:
- Eliciting and attending to the parents' concerns about their child's development
- Documenting and maintaining a developmental history
- Making accurate observations of the child
- Identifying the risk and protective factors
- Maintaining an accurate record and documenting the process and findings
A developmental screening is a brief assessment using a validated tool designed to identify children who should receive further assessment. A developmental screen is designed to evaluate whether an individual's development processes fall within a normal range of achievement according to age group. A developmental screening tool may be administered by appropriate office staff, however, the tool should be scored by the billing provider. If a developmental screening uncovers a potential developmental delay, the provider must make the appropriate referral to the appropriate provider for further evaluation. If a developmental delay is identified in a child ages 0-3 years old, the provider should refer to Colorado's Early Intervention Program. More information available at the Early Intervention Colorado website.
Developmental screens should be completed according to the Bright Futures periodicity schedule, at 9 months, 18 months, and 30 months of age. The assessment should consist of developmental history, observations, physical and developmental evaluation and assessment of developmental status. Health Education (anticipatory guidance including child development, healthy lifestyles, and accident and disease prevention).
Other Necessary Health Care Services
Additional health care services that are coverable under the Federal Medicaid program and found to be medically necessary to treat, correct or reduce illnesses and conditions discovered regardless of whether the service is covered in a state's Medicaid plan. It is the responsibility of states to determine medical necessity on a case-by-case basis (see medical necessity below for more information) and providers are to make requests for services that may not be covered by the state plan or by private insurance.
Diagnosis
A presumptive diagnosis may be made at the time of screening, but it is usually necessary to advise the member of the need for further diagnosis and treatment. Necessary treatments may be rendered by the PCP or MCO practitioner or by referral to an authorized Health First Colorado specialist.
Providers should make requests for services or items they feel best meets the child/youth needs even if they are not listed in the state plan as a benefit or the code is not showing as a benefit in the provider fee schedule.
Treatment
Necessary health care services must be made available for treatment of all physical and mental illnesses or conditions discovered by any screening and diagnostic procedures.
Under EPSDT, Health First Colorado beneficiaries are entitled to a broader scope of services than adults. Providers must make available or refer the member for the health care, treatment or other measures to correct or ameliorate defects and physical and mental illnesses or conditions discovered by EPSDT screening services.
Providers should make requests for services or items they feel best meets the child/youth needs even if they are not listed in the state plan as a benefit or the code is not showing as a benefit in the provider fee schedule.
Medical Necessity
All Health First Colorado coverable, medically necessary services must be provided even if the service is not available under the State plan to other Health First Colorado members. No arbitrary limitations on services are allowed, e.g., one pair of eyeglasses or 10 physical therapy visits per year.
Providers should consult the Rates and Fee Schedule web page to determine if the procedure code requires prior authorization. Medical necessity or a medically necessary service is defined as a good or service that will or is reasonably expected to prevent, diagnose, cure, correct, reduce, or ameliorate the pain and suffering, or the physical, mental, cognitive, or developmental effects of an illness, condition, injury, or disability. See Code of Colorado Regulations, Program Rules (10 CCR 2505-10.8.076.1.8), for the complete Medical Necessity Definition. For EPSDT, medical necessity includes a good or service that will or is reasonably expected to, assist the member to achieve or maintain maximum functional capacity in performing one or more Activities of Daily Living, and meets the criteria, Code of Colorado Regulations, Program Rules (10 CCR 2505-10.8.280.4.E.2).
To request services that a provider feels are medically necessary but are not currently covered, please visit the Billing Manuals section of the Department's website.
Health First Colorado makes the final determination of medical necessity and it is determined on a case-by-case basis. Provider recommendations will be taken into consideration but are not the sole determining factor in coverage. Colorado determines which treatment it will cover among equally effective, available alternative among equally effective treatments.
ColoradoPAR Prior Authorization Requests (PARs)
ColoradoPAR Peer-to-Peer and Reconsideration Process
If an EPSDT requested service or supply is denied or partially denied by the UM vendor the MD, DO, or APN who requested the PAR has the option to discuss the PAR over the phone in a process called a Peer-To-Peer review. If the Peer-To-Peer review still results in a denied or partially denied PAR, the EPSDT provider can work with the UM vendor two (2) options:
- PAR Reconsideration: A PAR Reconsideration is similar to a second opinion and must be requested by the EPSDT provider. A MD, DO, or APN who is different from the one who made the initial PAR denial will re-review the PAR along with the new information and make a final PAR decision. Additional documents not submitted with the original request may be submitted during the Reconsideration process.
- PAR Resubmission: Submit a new PAR that includes additional medical information needed for the PAR review.
The provider will be notified of the final PAR determination for all PARs reviewed by the UM vendor via the online PAR portal. The provider and member will receive the final PAR determination letter from the Department's fiscal agent. If the PAR is denied, the provider will also receive a detailed explanation of why the PAR was denied. A member who receives a denial notification letter has the option to submit a written request for an appeal to the Office of Administrative Courts.
EPSDT Medical Necessity Does NOT include:
- Experimental or investigational treatments,
- Services or items not in accordance with professionally recognized standards for health care in the United States, or
- Services primarily for caregiver or provider convenience
Services for which Colorado has a waiver are also not considered to be state plan benefits, and therefore are not a benefit under EPSDT. Items such as respite, in-home support services, and home modifications are examples of waiver services.
To request services that a provider feels are medically necessary but are not currently covered by the state plan, a prior authorization request must be completed as well as a letter of medical necessity. Both should be sent to the authorizing agent listed in Appendix D under the Appendices drop-down section on the Billing Manuals web page.
Benefits
Developmental, Depression, and Autism Screenings
Developmental
Health First Colorado enrolled children aged 0 - 4 (up to 59 months) following the 3 by 3 framework from the American Academy of Pediatrics (AAP). Three (3) screens per year for children aged 0 - 30 months.
Health First Colorado covers developmental screening for children ages 0 - 4 (up to 59 months), using a standardized, validated developmental screening tool (i.e., PEDS, Ages and Stages, etc.) at the child's periodic visits. In the absence of established risk factors or parental or provider concerns, the AAP recommends developmental screens at the 9-, 18-, and 30-months and not at every visit.
Depression
Health First Colorado covers an annual depression screening for individuals aged 11 and older, using a standardized, validated depression screening tool at the member's periodic visits. The department recommends the PHQ-9 but accepts other validated tools including the Edinburgh Postnatal Depression Scale, Columbia Depression Scale, Beck Depression Inventory, Kutcher Adolescent Depression Scale, etc. The exact frequency of validated, standardized screening depends on the concerns of the child's parents, adult member or the provider as to whether routine surveillance suggests the member may be at risk for depression.
The Depression benefit includes the option for reimbursing pediatricians or family medicine for screening new mothers for depression at well-child visits. As of July 2017, the Department will allow for up to three (3) screenings for the mother. Suggested screening times are at the 0 to 1-month visit, the 2-month visit, and either the 4-month or 6-month visit, however, providers may screen any time up to 12 months. Since other providers may also bill for the three postpartum depression screens, the Department recommends providers coordinate care with the member's obstetrician and any home visitor who provides services to the member. If possible, providers should bill under the mother's Medicaid ID, but, if not, the provider may bill for the screen under the child's Medicaid ID. The Department recommends the Edinburgh Postnatal Depression Scale (EPDS-10 or EPDS-2) but will accept the other validated tools listed above. If a behavioral health need is identified after screening, the pediatric provider should assist with referring the mother to a Regional Accountable Entity (RAE), or Regional Care Collaborative Organization (RCCO) provider. Resources for screening, discussing postpartum depression, and referring for positive screens can be found at the CDPHE Resource Hub for providers.
Autism
Health First Colorado covers autism screening for children aged 18- and 24-months, using a standardized, validated autism screening tool (i.e., M-CHAT, etc.) at the child's periodic visits. When an autism screen identifies a child as being at risk for an Autism Spectrum Disorder, an ASD Diagnostic Evaluation should follow.
Dental Benefits
A non-emergency oral examination, dental prophylaxis, and fluoride topical application once every six months are benefits of the EPSDT program. Health First Colorado recommends regular periodic examinations by a dentist with eruption of the first tooth or at age one, and continuing every six (6) months or as recommended by a dentist. Referral from the PCP is not required for EPSDT dental services.
Orthodontia is available for children who have been diagnosed with a severely handicapping malocclusion. More information can be found on the DentaQuest website.
Dentally necessary radiographs, restorations, endodontics, periodontics, prosthodontics and oral surgery are also benefits. Dental services are billed on the 2012 American Dental Association (ADA) claim form or the 837 D. Complete billing instructions for dental services are included in DentaQuest Provider Office Reference Manual (ORM) found under DentaQuest Resources section of the DentaQuest website. Health First Colorado dental providers can also call DentaQuest's Provider Relations/Services at 1-855-225-1731 (for TTY assistance, please call AT&T's TTY line at 711).
Hearing Assisted Device Benefits
Audiological benefits include identification, diagnostic evaluation, and treatment for children with hearing impairments. Benefits include hearing aids and other assisted devices, auditory training in the use of hearing aids, therapy for children with hearing impairments, and family-focused home-based early language intervention for children, (birth to three years of age), with hearing loss through the Colorado Home Intervention Program (CHIP).
Vision Care Benefits
Vision diagnostic and treatment services may be performed by an ophthalmologist or optometrist. Referral is not required for vision care. Single and multifocal vision lenses and frames, as well as repair or replacement of broken lenses or frames, are benefits of EPSDT and may be provided by an ophthalmologist, optometrist, or optician. Contact lenses are available in some medically necessary situations and require prior authorization.
Vision care services are billed on the CMS 1500 Health Insurance claim form or the 837P. Complete billing instructions for vision services are included in the vision billing manual.
Billing Guidelines
EPSDT Billing
Providers submitting claims electronically must use the 837P.
Providers submitting claims on paper must use the EPSDT paper claim form.
The EPSDT claim form is used by primary care providers who bill fee-for-service for EPSDT periodic screens.
The Department tracks the EPSDT periodic screens by procedure and diagnosis codes appropriate for the screen. Other children's health care services are billed on the CMS 1500, using national standard codes.
Providers must identify if a visit is a result of a referral from an EPSDT Screen
If a provider is seeing a child as a result of a referral from the EPSDT periodic screen for further diagnosis or treatment, the provider should enter a "Yes" in Box # L on the CMS 1500.
If the visit is a referral from an EPSDT periodic screen for further diagnosis and treatment, enter a "Yes" in the service line (Loop 2400, Segment SV1, Element SV111). It is important to identify these services as they are reported on the Annual EPSDT Participation Report (416) to the Centers for Medicare and Medicaid Services (CMS) along with the number of EPSDT periodic screens.
- Dental benefits are billed on the 2012 ADA claim form or the 837 D.
- Vision benefits are billed on the CMS 1500 claim form or 837P.
- If the child is ill, services related to the illness should be billed on the CMS 1500 claim form. An appointment for an EPSDT screening should be made at a later date.
- Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs) complete the UB-04 claim form for EPSDT-rendered services. Refer to the FQHC/RHC Billing Manual for specific UB- 04 billing instructions. FQHCs and RHCs use V72.0 to bill for the EPSDT Periodic Screen.
EPSDT benefits may include medically necessary covered benefits available for children enrolled in the Medical Assistance Program.
Procedure/HCPCS Codes Overview
The Department accepts procedure codes that are approved by the Centers for Medicare & Medicaid Services (CMS). The codes are used for submitting claims for services provided to Health First Colorado members and represent services that may be provided by enrolled certified Health First Colorado providers.
The Healthcare Common Procedural Coding System (HCPCS) is divided into two principal subsystems, referred to as level I and level II of the HCPCS. Level I of the HCPCS is comprised of Current Procedural Terminology (CPT), a numeric coding system maintained by the American Medical Association (AMA). The CPT is a uniform coding system consisting of descriptive terms and identifying codes that are used primarily to identify medical services and procedures furnished by physicians and other health care professionals.
Level II of the HCPCS is a standardized coding system that is used primarily to identify products, supplies, and services not included in the CPT codes, such as ambulance services and durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) when used outside a physician's office. Level II codes are also referred to as alpha-numeric codes because they consist of a single alphabetical letter followed by 4 numeric digits, while CPT codes are identified using 5 numeric digits.
HIPAA requires providers to comply with the coding guidelines of the AMA CPT Procedure Codes and the International Classification of Disease, Clinical Modification Diagnosis Codes. If there is no time designated in the official descriptor, the code represents one unit or session. Providers should regularly consult monthly bulletins on the Provider Services Bulletins web page. To receive electronic provider bulletin notifications, an email address can be entered into the Web Portal in the (MMIS) Provider Data Maintenance area or by completing and submitting a publication preference form. Bulletins include updates on approved procedures codes as well as the maximum allowable units billed per procedure. Always remember that any code or service can be requested, even if the code is not open in the fee schedule or listed in this or other billing manuals.
EPSDT Procedure Coding
| Periodic Screening: Preventive Medicine Codes* | |
| Procedure Code(s) | Description |
| 99381 - 99385 99391 - 99395 99431 99432 |
New Member (age specific) Established Member (age specific) History and examination Normal newborn care |
| Periodic Screening: Evaluation and Management Codes | |
| Procedure Code(s) | Description |
| 99203 - 99205 | New Member |
| 99214 - 99215 | Established Member |
| Note:These CPT-4 codes must be used in conjunction with the following Z codes: Z76.2, Z00.121, Z00.129, Z00.110, Z00.111, Z00.00-01, Z02.0, Z02.1, Z02.2, Z02.3, Z02.4, Z02.5, Z02.6, Z02.81, Z02.82, Z02.83, Z02.89, Z00.8, Z00.6, Z00.5, Z00.70, Z00.71. These codes must be used in conjunction with diagnosis codes for a well- child exam including 99202-99205, 99213-99215 |
|
| Inter-periodic Visit Codes | |
| Range 99201 - 99350 | |
| Note: Used in conjunction with the appropriate diagnosis codes excluding the well-child diagnosis codes: Z76.2, Z00.121, Z00.129, Z00.110, Z00.111, Z00.00-01, Z02.0 -Z02.6, Z02.81-Z02.83, Z02.89, Z00.5, Z00.6, Z00.70, Z00.71, Z00.8 | |
CMS 1500 Paper Claim Reference Table
The following paper form reference table shows required, optional, and conditional fields and detailed field completion instructions for the EPSDT claim form.
| CMS Field Number & Label | Field is? | Instructions | ||||||||||||||||||||||||||||||
| 1. Insurance Type | Required | Place an X in the box marked as Medicaid. | ||||||||||||||||||||||||||||||
| 1a. Insured's ID Number | Required | Enter the member's Health First Colorado seven-digit Medicaid ID number as it appears on the Medicaid Identification card. Example: A123456. | ||||||||||||||||||||||||||||||
| 2. Patient's Name | Required | Enter the member's last name, first name, and middle initial. | ||||||||||||||||||||||||||||||
| 3. Patient's Date of Birth/Sex | Required | Enter the member's birth date using two digits for the month, two digits for the date, and two digits for the year. Example: 070114 for July 1, 2014. Place an X in the appropriate box to indicate the sex of the member. |
||||||||||||||||||||||||||||||
| 4. Insured's Name | Not Required | |||||||||||||||||||||||||||||||
| 5. Patient's Address | Not Required | |||||||||||||||||||||||||||||||
| 6. Client Relationship to Insured | Conditional | Complete if the member is covered by a commercial health care insurance policy. | ||||||||||||||||||||||||||||||
| 7. Insured's Address | Not Required | |||||||||||||||||||||||||||||||
| 8. Reserved for NUCC Use | Not Required | |||||||||||||||||||||||||||||||
| 9. Other Insured's Name | Conditional | If field 11d is marked YES, enter the insured's last name, first name and middle initial. | ||||||||||||||||||||||||||||||
| 9a. Other Insured's Policy or Group Number | Conditional | If field 11d is marked "YES", enter the policy or group number. | ||||||||||||||||||||||||||||||
| 9b. Reserved for NUCC Use | ||||||||||||||||||||||||||||||||
| 9c. Reserved for NUCC Use | ||||||||||||||||||||||||||||||||
| 9d. Insurance Plan or Program Name | Conditional | If field 11D is marked "YES", enter the insurance plan or program name. | ||||||||||||||||||||||||||||||
| 10a-c. Is patient's condition related to? | Not Required | |||||||||||||||||||||||||||||||
| 10d. Reserved for Local Use | ||||||||||||||||||||||||||||||||
| 11. Insured's Policy, Group or FECA Number | Not Required | |||||||||||||||||||||||||||||||
| 11a. Insured's Date of Birth, Sex | Not Required | |||||||||||||||||||||||||||||||
| 11b. Other Claim ID | Not Required | |||||||||||||||||||||||||||||||
| 11c. Insurance Plan Name or Program Name | Not Required | |||||||||||||||||||||||||||||||
| 11d. Is there another Health Benefit Plan? | Conditional | When appropriate, place an "X" in the correct box. If marked "YES", complete 9, 9a and 9d. | ||||||||||||||||||||||||||||||
| 12. Patient's or Authorized Person's signature | Required | Enter "Signature on File", "SOF", or legal signature. If there is no signature on file, leave blank or enter "No Signature on File". Enter the date the claim form was signed. |
||||||||||||||||||||||||||||||
| 13. Insured's or Authorized Person's Signature | Not Required | |||||||||||||||||||||||||||||||
| 14. Date of Current Illness Injury or Pregnancy | Not Required | |||||||||||||||||||||||||||||||
| 15. Other Date Not | Not Required | |||||||||||||||||||||||||||||||
| 16. Date Patient Unable to Work in Current Occupation | Not Required | |||||||||||||||||||||||||||||||
| 17. Name of Referring Physician | Conditional | |||||||||||||||||||||||||||||||
| 18. Hospitalization Dates Related to Current Service | Conditional | Complete for services provided in an inpatient hospital setting. Enter the date of hospital admission and the date of discharge using two digits for the month, two digits for the date and two digits for the year. Example: 070116 for July 1, 2016. If the member is still hospitalized, the discharge date may be omitted. This information is not edited. | ||||||||||||||||||||||||||||||
| 19. Additional Claim Information | Conditional | |||||||||||||||||||||||||||||||
| 20. Outside Lab? $ Charges |
Conditional | Complete if all laboratory work was referred to and performed by an outside laboratory. If this box is checked, no payment will be made to the physician for lab services. Do not complete this field if any laboratory work was performed in the office. Practitioners may not request payment for services performed by an independent or hospital laboratory. |
||||||||||||||||||||||||||||||
| 21. Diagnosis or Nature of Illness or Injury | Required | Enter at least one but no more than twelve diagnosis codes based on the member's diagnosis/condition. Enter applicable ICD-10 indicator. |
||||||||||||||||||||||||||||||
| 22. Medicaid Resubmission Code | Conditional | List the original reference number for resubmitted claims. When resubmitting a claim, enter the appropriate bill frequency code in the left- hand side of the field. 7 - Replacement of prior claim 8 - Void/Cancel of prior claim This field is not intended for use for original claim submissions. |
||||||||||||||||||||||||||||||
| 23. Prior Authorization | Not Required | |||||||||||||||||||||||||||||||
| 24. Claim Line Detail | Information | The paper claim form allows entry of up to six detailed billing lines. Fields 24A through 24J apply to each billed line. Do not enter more than six lines of information on the paper claim. If more than six lines of information are entered, the additional lines will not be entered for processing. Each claim form must be fully completed (totaled). Do not file continuation claims (e.g., Page 1 of 2). |
||||||||||||||||||||||||||||||
| 24A. Dates of Service | Required | The field accommodates the entry of two dates: a From date of services and a To date of service. Enter the date of service using two digits for the month, two digits for the date and two digits for the year. Example: 010116 for January 1, 2016.
All dates of service must be the same date as screening. |
||||||||||||||||||||||||||||||
| 24B. Place of Service | Required | Enter the Place of Service (POS) code that describes the location where services were rendered. Health First Colorado accepts the CMS place of service codes.
|
||||||||||||||||||||||||||||||
| 24C. EMG | Conditional | Enter a Y for YES or leave blank for NO in the bottom, unshaded area of the field to indicate the service is rendered for a life- threatening condition or one that requires immediate medical intervention. If a Y for YES is entered, the service on this detail line is exempt from co-payment requirements. |
||||||||||||||||||||||||||||||
| 24D. Procedures, Services, or Supplies | Required | Enter the HCPCS procedure code that specifically describes the service for which payment is requested. All procedures must be identified with codes in the current edition of Physicians Current Procedural Terminology (CPT). CPT is updated annually. HCPCS Level II Codes The current Medicare coding publication (for Medicare crossover claims only). Only approved codes from the current CPT or HCPCS publications will be accepted. |
||||||||||||||||||||||||||||||
| 24D. Modifier | Conditional | Enter the appropriate procedure-related modifier that applies to the billed service. Up to four modifiers may be entered when using the paper claim form.
|
||||||||||||||||||||||||||||||
| 24E. Diagnosis Pointer | Required | Enter the diagnosis code reference letter (A-L) that relates the date of service and the procedures performed to the primary diagnosis. At least one diagnosis code reference letter must be entered. When multiple services are performed, the primary reference letter for each service should be listed first, other applicable services should follow. This field allows for the entry of 4 characters in the unshaded area. |
||||||||||||||||||||||||||||||
| 24F. $ Charges | Required | Enter the usual and customary charge for the service represented by the procedure code on the detail line. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. Some CPT procedure codes are grouped with other related CPT procedure codes. When more than one procedure from the same group is billed, special multiple pricing rules apply. The base procedure is the procedure with the highest allowable amount. The base code is used to determine the allowable amounts for additional CPT surgical procedures when more than one procedure from the same grouping is performed. Submitted charges cannot be more than charges made to non-Health First Colorado covered individuals for the same service. Do not deduct Health First Colorado co- payment or commercial insurance payments from the usual and customary charges. |
||||||||||||||||||||||||||||||
| 24G. Days or Units | Required | Enter the number of services provided for each procedure code. Enter whole numbers only- do not enter fractions or decimals. |
||||||||||||||||||||||||||||||
| 24H. EPSDT/Family Plan | Conditional | EPSDT (shaded area) For Early & Periodic Screening, Diagnosis, and Treatment related services, enter the response in the shaded portion of the field as follows:
Not Required |
||||||||||||||||||||||||||||||
| 24I. ID Qualifier | Not Required | |||||||||||||||||||||||||||||||
| 24J. Rendering Provider ID # | Required | Enter the NPI number of the provider performing the service. | ||||||||||||||||||||||||||||||
| 25. Federal Tax ID Number | Not Required | |||||||||||||||||||||||||||||||
| 26. Patient's Account Number | Optional | Enter information that identifies the member or claim in the provider's billing system. Submitted information appears on the Remittance Advice (RA). | ||||||||||||||||||||||||||||||
| 27. Accept Assignment? | Required | The accept assignment indicates that the provider agrees to accept assignment under the terms of the payer's program. | ||||||||||||||||||||||||||||||
| 28. Total Charge | Required | Enter the sum of all charges listed in field 24F. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. | ||||||||||||||||||||||||||||||
| 29. Amount Paid | Conditional | Enter the total amount paid by Medicare or any other commercial health insurance that has made payment on the billed services. Do not use commas when reporting dollar amounts. Enter 00 in the cents area if the amount is a whole number. |
||||||||||||||||||||||||||||||
| 30. Rsvd for NUCC Use | ||||||||||||||||||||||||||||||||
| 31. Signature of Physician or Supplier Including Degrees or Credentials | Required | Each claim must bear the signature of the enrolled provider or the signature of a registered authorized agent. Each claim must have the date the enrolled provider or registered authorized agent signed the claim form. Enter the date the claim was signed using two digits for the month, two digits for the date and two digits for the year. Example: 070116 for July 1, 2016. |
||||||||||||||||||||||||||||||
| 32. Service Facility Location Information 32a- NPI Number 32b- Other ID # |
Required | Enter the name, address and ZIP code of the individual or business where the member was seen or service was performed in the following format: 1st Line Name 2nd Line Address 3rd Line City, State and ZIP Code If the Provider Type is not able to obtain an NPI, enter the eight-digit Health First Colorado provider number of the individual or organization. |
||||||||||||||||||||||||||||||
| 33. Billing Provider Info & Ph # |
Required | Enter the name of the individual or organization that will receive payment for the billed services in the following format: 1st Line Name 2nd Line Address 3rd Line City, State and ZIP Code |
||||||||||||||||||||||||||||||
| 33a- NPI Number | Required | |||||||||||||||||||||||||||||||
| 33b- Other ID # | If the Provider Type is not able to obtain an NPI, enter the eight-digit Health First Colorado provider number of the individual or organization. | |||||||||||||||||||||||||||||||
CMS 1500 EPSDT Claim Example
Timely Filing
For more information on timely filing policy, including the resubmission rules for denied claims, please see the General Provider Information manual.
EPSDT Revisions Log
| Revision Date | Section/Action | Made by |
| 12/1/2016 | Manual revised for interChange implementation. For manual revisions prior to 12/01/2016 Please refer to Archive. | HPE (now DXC) |
| 12/27/2016 | Updates based on Colorado iC Stage II Provider Billing Manuals Comment Log v0_2.xlsx. | HPE (now DXC) |
| 1/10/2017 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_3.xlsx | HPE (now DXC) |
| 1/19/2017 | Updates based on Colorado iC Stage II Provider Billing Manual Comment Log v0_4.xlsx | HPE (now DXC) |
| 1/26/2017 | Updates based on Department 1/20/2017 approval email | HPE (now DXC) |
| 5/22/2017 | Updates based on Fiscal Agent name change from HPE to DXC | DXC |
| 7/19/2017 | Updates pertaining to the depression screening benefit | HCPF |
| 6/22/2018 | Removal of PAR which could be found in general manual, updated billing to point to general manual, updated timely filing to point to general manual, replace BHO with RAE | HCPF |
| 12/21/2018 | Clarification to signature requirements | HCPF |
| 3/18/2019 | Clarification to signature requirements | HCPF |
| 7/11/2019 | Updated Appendices links and verbiage | DXC |
| 12/13/2019 | Converted to web page | HCPF |
| 09/10/2020 | Added Line to Box 32 under the CMS 1500 Paper Claim Reference Table | HCPF |